Overview
A total of 148 people completed the women’s health outpatient survey, which ran from 20 March to 20 April 2026.
We ran this survey to understand people’s experiences, expectations and views of women’s health services, to help inform how care for gynaecological and wider women’s health concerns can be improved across south west London. The focus is on how people move through the pathway, from first seeking advice in primary care or community settings, through to referral, specialist assessment and treatment, and whether care is being delivered in the right place, at the right time, with the right support.
Women’s health services cover a wide range of needs, including contraception, menopause care, heavy and painful periods, pelvic pain, bladder and pelvic floor problems, and other gynaecological conditions. Care can be provided across multiple settings, including GP practices, community services and hospital outpatient clinics, depending on the complexity of need. The pathway often begins in primary care, with onward referral to specialist services where symptoms are persistent, complex or require further investigation.
Alongside this, there is ongoing development of more joined-up models of care, including the potential use of women’s health hubs in community settings. These hubs would be designed to bring together different services and professionals in one place, supporting more coordinated care and improving access. They may offer services such as menopause support, coil fitting and treatment for common gynaecological conditions, as well as enabling quicker access to specialist advice and reducing the need for hospital referral in some cases.
Most respondents had direct experience of women’s health services, with 72% reporting that they had accessed care as a patient. A further 4% responded as a carer or family member, 14% had not yet accessed services but expected to in the future and 10% had no direct experience but wanted to share their views.
Responses reflected experiences across primary care, community services and hospital-based care. Overall, experiences were mixed. While some people described positive, supportive care, many highlighted challenges including delays in accessing appointments, inconsistent communication and experiences of not feeling listened to, believed or taken seriously.
Methodology
We developed these surveys with ICB clinical leads and Acute Provider Collaborative colleagues to better understand experiences of women’s health services. It was widely shared through partner organisations, including voluntary and community sector networks, who distributed it within their local communities. It was also promoted through paid for adverts across organisational social media channels to reach people with experience of women’s health services and outpatient care across South West London.
The survey was open to adults who had used outpatient services in the past two years or who may need to use them in future.
As with all open surveys, findings are not representative of the wider population and reflect the views of those who chose to respond. The sample is self-selecting and likely to be influenced by individuals with stronger experiences or interest in the topic.
The survey had a higher proportion of respondents identifying as White British/White English and female, meaning some communities may be under-represented.
Responses were also gathered online, which may have created barriers for some groups, particularly those with limited digital access or lower health literacy.
Summary of key findings
- Experiences of using women’s health services were very mixed – experiences varied significantly. While some people described positive and supportive care, others reported feeling dismissed, not listened to, or unsupported.
- Long waiting times and difficulty getting appointments causes frustration and stress. There are challenges accessing timely support, including GP appointments, referrals, investigations and specialist care. Long waits led to frustration, anxiety and sometimes worsening symptoms.
- Feeling listened to makes a huge difference – a consistent theme throughout was the importance of healthcare professionals, listening, showing empathy and involving people in decisions about their care. This led to positive experiences of feeling heard and supported. Those negative experiences were more associated with feeling dismissed or rushed.
- Communication between services and patients could be improved. Respondents described confusion around referral pathways, waiting times, treatment options and available support. Some people reported receiving conflicting advice from different professionals and wanted clearer, more accessible information throughout their care.
- People want women’s health services to feel more joined up and easier to navigate. Many respondents wanted services to feel more coordinated and easier to navigate. People valued continuity of care, easier access to specialist support, and more holistic approaches that considered both physical and emotional wellbeing
Summary of key questions
- Equalities, inclusion and safety. Across all questions, people said women’s health services should be inclusive, culturally safe and trauma‑informed. People described experiences of bias, stigma, language barriers, and feeling dismissed due to age, ethnicity, disability, trauma history or communication style. Some emphasised the need for female clinicians for intimate care, while others felt that over‑gendered language can be exclusionary.
- Experiences of accessing support. Experiences varied considerably across the pathway. Positive experiences were associated with rapid referrals, coordinated care, and clear communication, while negative experiences focused on long waits, cancelled appointments, poor communication and difficulty accessing follow‑up support. Many people felt they had to chase referrals, appointments or results themselves.
- Confidence in community‑based or hub‑based care. People were generally open to community clinics or women’s health hubs if they were staffed by clinicians with genuine women’s health expertise and had clear escalation routes. Confidence dropped for complex or unexplained conditions, with concerns about delayed escalation, misdiagnosis, and loss of specialist oversight. Waiting times and communication while waiting.
- Expectations after contacting a GP. People expected active investigation and clear next steps following initial contact. This included timely referrals, access to specialist advice, diagnostic support, treatment plans and reassurance that concerns were being taken seriously. Respondents also expected better coordination between GP, community and hospital services.
- Reassurance and ongoing support. Confidence increased when clinicians clearly explained conditions, ruled out serious illness, and provided ongoing support or follow‑up arrangements. Anxiety was linked to uncertainty, worsening symptoms, lack of updates and feeling unsupported while waiting. People particularly valued continuity and easy re‑access to services if symptoms changed.
- Views on different models of care. Many respondents were open to GP‑led specialist advice pathways, community clinics and rapid‑advice models where these improved speed and convenience. However, people wanted reassurance that specialist oversight would remain, and that new approaches would not reduce quality or delay diagnosis.
- Fairness of prioritisation and pathway management. Most respondents accepted that appointments should be prioritised according to clinical need but wanted greater transparency around how decisions are made. People felt systems should allow worsening symptoms to be reassessed quickly and wanted clearer communication about referral status and expected waiting times.
- Barriers to accessing services. Key barriers included previous poor experiences, work commitments, carer responsibilities, mobility and transport issues, language barriers, and stigma. Some said gendered language made them feel unwelcome; others said lack of female clinicians made them feel unsafe
- Support needed while waiting. People wanted someone to contact, clear waiting time information, regular updates, symptom management advice, and access to community tests. Qualitative responses emphasised monitoring, emotional support, ability to escalate, and support with work and daily life.
Who we heard from?
Most respondents also provided demographic information, although some people chose not to answer every question, which meant that the total has varied across this section.
The survey was predominantly completed by women aged 45–59, with responses received from residents across all south west London boroughs. Two people identified as male, one as non-binary and two preferred not to share their gender. 98% of respondents reported that their sex at birth matches their current sex.
The largest number of responses came from Wandsworth (31), Merton (27) and Richmond (25). Sutton had 21 responses, Croydon 20 and Kingston 16. Five people completed the survey who lived out of these boroughs. Those areas included Lambeth and Surrey.
Respondents came from a range of ethnic backgrounds, although responses were higher among White British and White English participants compared to other groups. Smaller numbers of responses were received from Black, Asian and mixed ethnic communities.
Just under half of respondents answered the question on long-term health conditions or disabilities. 35% of respondents reported mental ill health, followed by a learning disability or long-term condition.
Many people chose “other” health conditions. These included things like joint and mobility problems, neurological or autoimmune conditions, chronic pain, reproductive health issues such as endometriosis, and metabolic conditions like an underactive thyroid. Some people also mentioned being neurodivergent or autistic and others said they had more than one condition at the same time. A small number of people said they did not have any disability or long‑term conditions.
Detailed insight
Where have people accessed care?
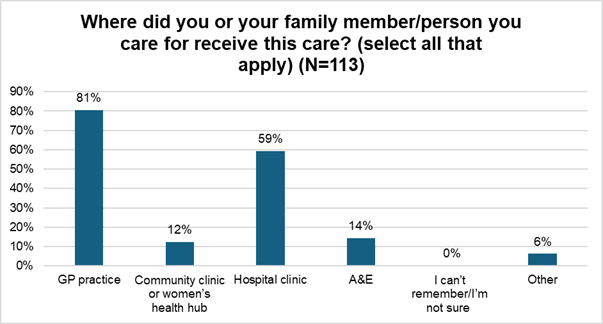
Out of the 113 people who answered this question, 72% of people have used women’s health services in the past two years. A small number (4%) accessed these services as a carer or family member rather than as a patient themselves. 14% haven’t used the services yet but expect they may need them in future and 10% hadn’t used them but wanted to share their thoughts on women’s health services.
Of those who’ve used women’s health services, 81% accessed care through their GP. That makes the GP practice the main point of contact for women’s health.
Nearly 60% also went to hospital clinics, 14% had used A&E and 12% had used women’s health hubs or community clinics.
Alongside NHS services, some people also described accessing care through private or alternative routes, including private ultrasound, MRI scanning, private menopause specialists, health insurance or privately funded hormone replacement therapy (HRT) support. In some cases, said they have used private services due to difficulty accessing NHS appointments, including one example of a referral waiting six months without an appointment being received. Other individual experiences included care accessed through occupational health or home-based support.
Experience of gynaecology and womens health services
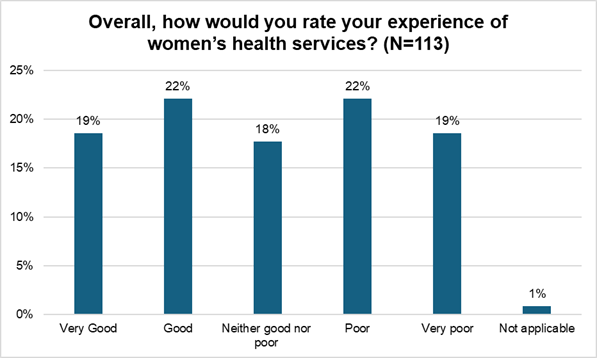
Women’s experiences of health services varied. About 41% said their experience was good or very good, and almost the same number said it was poor or very poor. Another 18% felt their experience was somewhere in the middle, neither good nor bad.
What is working well?
When a clinician, listens and responds with empathy, it really changes how people feel and experience a service. Positive experiences were shared when GPs took time to listen, acknowledged symptoms and made referrals to the appropriate setting. Feeling believed and supported at the first point of contact made a significant difference, particularly for those who had previously struggled to be listened to by a health professional.
“GP listened to my issues and understood what I needed”
Being referred and treated quickly can have a significant impact on an individual’s outcome. When services work effectively, people experience quick referrals, fast access to diagnostics and timely treatment, including urgent referral timeframes and progression from referral to surgery within weeks. The difference in speed of access can have a major impact on people’s experiences and outcomes, with timely pathways often described as reassuring and in some cases lifesaving.
“The speed that I was dealt with. 4 weeks from referral to surgery. Saved my life.”
Specialist clinics and hospital teams were praised for their expertise, clear communication and respectful approach. People valued being seen by clinicians who understood their condition, explained options clearly, and provided high-quality, patient-centred care.
“They knew their stuff and took me seriously, listened, empathised and discussed options with me.”
Clear and accessible communication and involvement in decision-making can improve experience.
Positive experiences included being given accessible and detailed information about treatment options, understanding what tests were for and being involved in decisions about care. This helped people feel more in control and confident in managing their health.
“I was given information about treatment options and allowed to choose…”
Seeing the same clinician builds trust and confidence.
Where people experienced consistent care from the same clinician or team, this helped to build trust and feel listened to. It also helped make sure that care was tailored to the individual and could be changed, if needed.
“The referral was requested and sent… regular follow ups, medication reviews, seeing the same person…”
Flexible and accessible services support better engagement with care.
Examples of good practice included weekend appointments, flexible scheduling and services that reduced the need to take time off work. Easy access to appointments, including walk-in or local clinics, was also seen as a positive.
“A hospital appointment was offered for a Saturday, so I didn’t have to take time off work.”
Kind, respectful and professional staff make a significant difference to overall experience. Across many responses, staff attitudes were highlighted as a key factor. Friendly, approachable and compassionate clinicians and nurses helped create a comfortable environment, particularly when discussing sensitive issues.
“Nursing team… lovely, approachable, friendly.”
What needs to improve?
Access to care can be a challenge, with long waits for appointments, referrals and treatment. Waiting times were one of the most consistent concerns, including GP appointments, specialist referrals, diagnostic tests and surgery. Delays of months or years were reported, even for severe or worsening symptoms. These delays were described as having significant physical, emotional and wider life impacts, including worsening conditions, loss of education or work opportunities and prolonged pain.
Respondents also described delays after referral, including long waits for specialist appointments, cancelled or postponed appointments and in some cases discharge without any appointment taking place. Difficulties with triage systems and administrative processes were also highlighted, including unclear routes for accessing appointments, difficulty navigating booking systems, and repeated delays in receiving care after initial referral. Some respondents also described multiple cycles of referral and waiting, with limited clarity on timelines or next steps.
Women do not feel their symptoms are taken seriously, particularly at first point of contact. Many people described feeling dismissed, not believed, or having their symptoms minimised as “normal”, anxiety-related, or something to “put up with”. This was particularly evident in relation to pain, menopause symptoms, endometriosis, fibroids, postnatal health, and postnatal mental health. Several people felt they had to repeatedly push or “fight” for referrals, with some only receiving appropriate care after years of being ignored. Some felt that women’s experiences are still not given equal weight, with reports of outdated attitudes in how symptoms are interpreted and managed.
There were also calls for greater respect, reassurance, and belief in women’s reported symptoms, with respondents emphasising the importance of “believing women” when they seek help for pain and health concerns.
“Stop assumptions that women are hysterical/exaggerating… I was told I should put up with pain because ‘it takes longer to heal as you get older’”
People reported perceived gaps in knowledge and confidence in women’s health within primary care, particularly in relation to menopause, perimenopause and other gynaecological conditions. A recurring issue was inconsistent or limited understanding among some GPs, with accounts of people receiving conflicting or incorrect advice, inappropriate prescriptions, or being directed towards treatments such as antidepressants without underlying physical causes being fully explored.
Some respondents also described gaps in postnatal care, fertility care, and longer-term reproductive health management, including delayed follow-up, lack of clarity on ongoing responsibility for care, and limited recognition of complex or long-term symptoms.
Some respondents described negative experiences during clinical examinations, where they felt the GP lacked sufficient experience in carrying out relevant procedures. In one case, this resulted in a painful and distressing experience where a second GP had to be called to complete the examination. This contributed to views that gynaecological care should be delivered by appropriately trained clinicians and that patient preference, including clinician gender where appropriate, should be better considered.
“GP knowledge- given conflicting and wrong advice by different GPs.”
Pathways feel disjointed, with poor coordination and lack of accountability across services. Many people described fragmented care, where responsibility sits between GP and hospital services, leading to gaps in monitoring, follow-up and treatment. Poor communication between services, missing records, and unclear clinical ownership left people feeling unsupported and having to manage their own care.
Respondents also described a lack of continuity after appointments or procedures, including limited or no follow-up communication, missing letters or updates, and uncertainty about treatment plans. Some patients reported needing to repeatedly chase services for information or personally collate their own records to ensure appropriate care decisions were made.
“I want joined up care – I don’t want to have to read my patient notes to understand my own complex case”
Some women reported turning to private healthcare after feeling unable to access timely or appropriate NHS support. Several respondents described paying privately for scans, specialist consultations, surgery or menopause care after experiencing delays, dismissal or barriers within NHS services. In some cases, private diagnoses or investigations were later used to support NHS care pathways, raising concerns about inconsistency in how information is valued across systems.
“I was finally listened to when I requested a referral to private care.”
Perceived gender bias and dismissal of symptoms. Some respondents described experiences where their symptoms were not fully believed or were initially attributed to factors such as mental health, weight, or normal menstrual changes. This was particularly raised in relation to conditions such as endometriosis, menopause and perimenopause, where symptoms were sometimes minimised or not appropriately investigated. Some respondents also described broader concerns about gendered assumptions in how women’s symptoms are assessed and treated.
“I’m early peri-menopausal, just turned 40 – mother completed meno at 37 – very early. GP refused to believe me”
Pain management, procedures and trauma-informed care. Concerns were raised about the management of pain during gynaecological procedures, particularly where pain was not adequately anticipated or managed. Some respondents described procedures being attempted without sufficient pain relief or consideration of individual circumstances, resulting in significant distress and, in some cases, procedures being aborted.
Experiences also highlighted a lack of sensitivity to trauma, neurodiversity, and communication needs during care delivery, with some respondents feeling that their circumstances were not fully understood or adapted for in clinical settings. Some also described broader concerns about how pain is communicated in advance of procedures.
“A gynaecologist tried to insert a Mirena coil without anaesthesia… the attempt had to be aborted due to the severity of her pain.”
Do people feel listened to?
When people were asked whether they felt their concerns were listened to and taken seriously by healthcare professionals, opinions were evenly split. Half said yes, they felt heard, while the other half said no, they didn’t feel their concerns were taken seriously.
When asked to share more details, people said:
- Women’s health concerns are not always taken seriously. People described feeling dismissed, not believed, or having symptoms minimised, resulting in delayed diagnosis and treatment. Some felt assumptions were made based on their age, while others reported having to repeatedly advocate for themselves before receiving appropriate care.
- Poor communication leaves people feeling unsupported. People reported poor communication from healthcare professionals, including condescending language, lack of follow-up, and inadequate explanations.
- A lack of trauma-informed and person-centred care can cause distress. Several participants described healthcare experiences that failed to recognise their emotional, trauma, or support needs, particularly during intimate procedures. This led to anxiety, distress, and reluctance to engage with future care.
- Delays and barriers to accessing care can leave people without the support they need. This included long waits, cancelled appointments, difficulties accessing treatment and being forced to seek private care when NHS services were unavailable or unresponsive.
Views on accessing urgent care
When people were asked if they had gone to A&E in the past two years because of a women’s health issue, such as severe pain or heavy bleeding, most said no. Only 15% had attended A&E for this reason, while 85% had not.
Among those who attended, experiences highlighted that A&E is often used when symptoms escalate due to delays in earlier care, particularly for severe pain, heavy bleeding and acute gynaecological symptoms.
- Avoiding A&E until symptoms become extreme. People said they try to avoid A&E because of long waits and delays. However, when there’s no other choice, they attend, often while in severe pain or heavy bleeding.
- Feeling dismissed or not listened to. When people did use A&E, many felt their concerns weren’t taken seriously. Symptoms were sometimes attributed to constipation, UTIs, or “just a heavy period” despite patients insisting otherwise. Some were denied scans, refused IUD removal, or discharged without investigation.
- Lack of dignity during heavy bleeding. Women described sitting on INCO pads in busy waiting rooms and having to change them publicly. One person said she sat for hours in a blood‑soaked dress waiting for the pharmacy to open.
- Poor pain and symptom management. People with chronic or recurrent pain said their management didn’t improve despite multiple admissions. They felt this was due to poor coordination between digital systems and patient records.
- No clear care pathway. Many felt they were bounced between GP, A&E, and clinics without a clear plan or follow‑up.
- Turning to private care. Some said they had to seek private treatment after NHS services refused investigations.
Expectations and reassurance
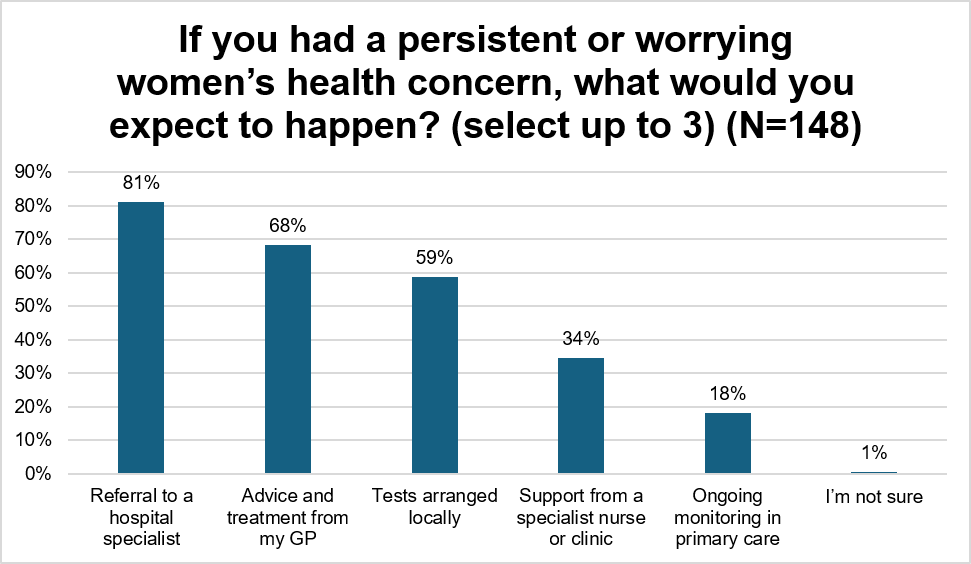
When people have a persistent or worrying women’s health concern, here’s what they expect to happen:
81% expect to be referred to a hospital specialist. 68% also expect their GP to give them advice and treatment, and 59% expect tests to be arranged locally.
Fewer people (34%) expect to see a specialist nurse and only 18% expect ongoing monitoring in primary care. Only 1% of people were not sure what to expect.
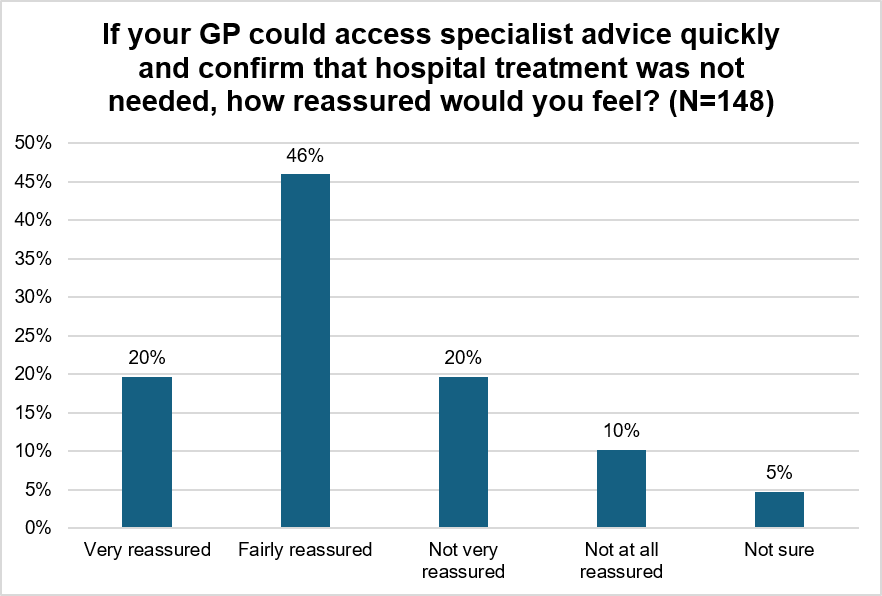
What would help with reassurance?
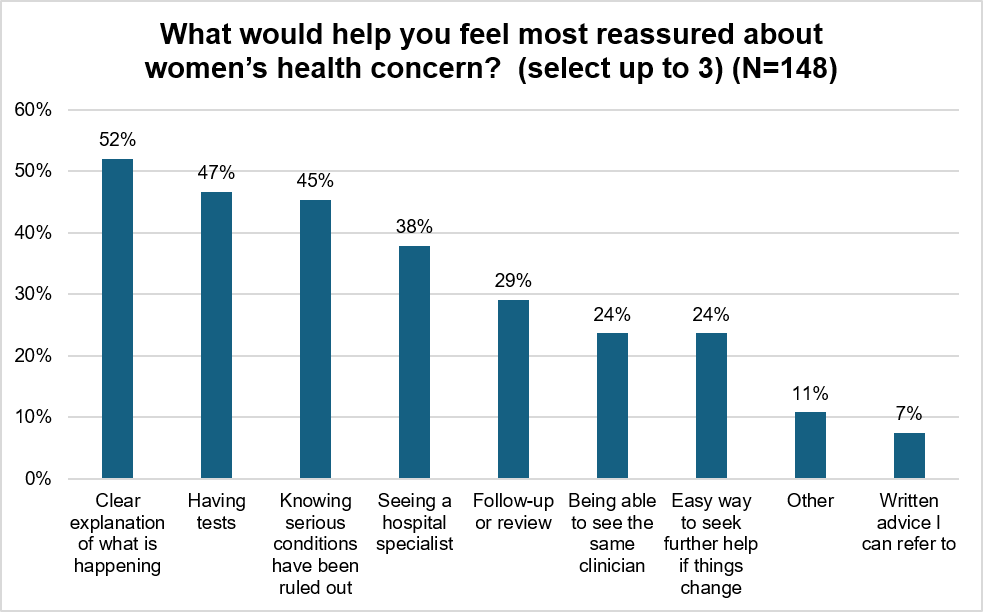
When asked what other support could help people feel more reassured, they said:
- More choice of female GPs – people want easier access to women doctors every day.
- Direct access to specialists – quicker ways to contact consultants already involved in care, not months‑long waits.
- Not being dismissed – especially by male doctors.
- Proper investigation of symptoms – tests for physical causes rather than assumptions or stereotypes.
- GPs trained in women’s health – including menopause, endometriosis, PCOS, POI and other female‑specific conditions.
- Quicker appointments – no long waits for routine or specialist care.
- Confidence in specialist expertise – reassurance that gynaecologists and surgeons are fully trained, especially for complex conditions like endometriosis.
- Clear information on treatment rights – including the right to alternative providers if NHS waiting‑time limits are exceeded.
- Concerns not dismissed as anxiety – recognition of patients’ own knowledge of their bodies.
- Access to wider support services – endocrinology, dietetics, nutrition, counselling, and imaging specialists trained to detect complex conditions.
- Up‑to‑date GP knowledge – especially on female‑specific conditions and modern diagnostic pathways.
Views on alternative models of care
Views on different ways of delivering care
Some women’s health services could potentially be delivered differently, for example: Bringing together services such as contraception, menopause care and treatment for heavy periods in local women’s health hubs Offering more appointments in community clinics rather than hospital settings GPs getting rapid advice from specialists so some women may not need to wait for a hospital referral. Where clinically appropriate, how comfortable would you feel with these approaches?
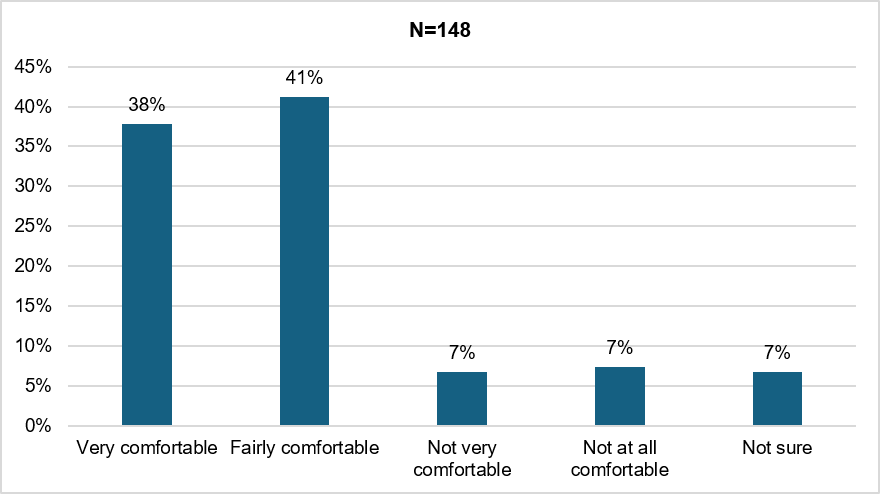
This section summarises the concerns people raised about these proposed approaches. While many welcomed the idea of improving access to women’s health support, respondents highlighted a few risks and uncertainties that would need to be addressed for the model to work well.
- Worry about lack of specialist expertise. People fear hubs will be staffed by generalists rather than true women’s health specialists.“They must be specialists not generalist gynaecologists or gynae nurses.”
- Concern about being dismissed or not taken seriously. A major fear is that symptoms will be minimised, mislabelled as anxiety, or not investigated properly. “Really serious conditions are often ignored as ‘anxiety’ or ‘panic’ or ‘hysteria’ even in hospital.”
- Lack of confidence in GP knowledge and training. Many feel GPs do not have the depth of knowledge needed for complex women’s health issues.“GPs are already dismissive of female issues… I have no confidence in GPs.”
- Fear that hubs could delay or block access to specialists. People worry these models will create another layer of triage and slow down referrals. “My worry is that they would be used to delay specialist referrals desperately needed for things like endometriosis.”
- Concern that serious conditions could be missed. Without proper diagnostics and specialist review, people fear life‑changing conditions will go undetected.“Something serious might be missed.”
- Need for proper diagnostic tools (scans, blood tests, imaging). Confidence depends on access to the right equipment, not just advice “A quick ultrasound can tell the difference between a benign cyst and a life‑threatening abscess.”
- Anxiety about fragmented, confusing or inconsistent care. People worry that moving care into hubs will make the system harder to navigate“Moving care around between different places can just make it more confusing and harder to speak to someone who is able to help you.”
- Concerns about staffing, funding and capacity. There is scepticism about whether hubs can work when services are already stretched. “Who will staff the community women’s health hubs as there is already a lack of gynae staff?”
- Fears about unequal treatment, discrimination and language barriers. Some women, especially those who are migrants, non‑native English speakers, or from marginalised groups fear they will not be listened to or treated with respect.“Probably because I am foreign, I was not treated seriously.”
- Worries about pregnancy‑related care and missed opportunities. Some women describe symptoms being minimised or misunderstood, leading to harm. “I needed scan. When it was fine was too late to heal… I lost the last chance to have a baby.”
- Concern about hygiene, empathy and basic care standards. Some experiences raise fears about safety, dignity and compassion. “I felt uncomfortable with the staff’s attitude… gloves are not always used.”
- Accessibility concerns, travel, timing, and record‑sharing. People want hubs to be genuinely local, with joined‑up records and flexible appointments. “What seems ‘local’ to the NHS often isn’t actually accessible to me.”
There would be support for new approaches if:
- Clinicians with women’s health expertise were available. People want to be seen by clinicians who genuinely understand women’s health conditions, rather than generalists.
“I would want to know that the medical practitioner I saw was specialist enough.”
- Care is properly coordinated and joined up. People want reassurance that care is connected, with clear responsibility for ongoing management and continuity, including that “all notes are in one place in my patient record.”
- Tests, investigations are escalated when needed. People want reassurance that symptoms will be properly investigated and not delayed or dismissed. This includes access to scans and diagnostic tests, with appropriate escalation to specialists where required to avoid missed or delayed diagnoses.
- Any new model of care must include specialist expertise, shorter waiting times and clear pathways and referrals when hospital care is needed. Without those, people worry that serious conditions could be missed. “If I had access to specialist units that would be a game changer.”
Barriers to accessing services
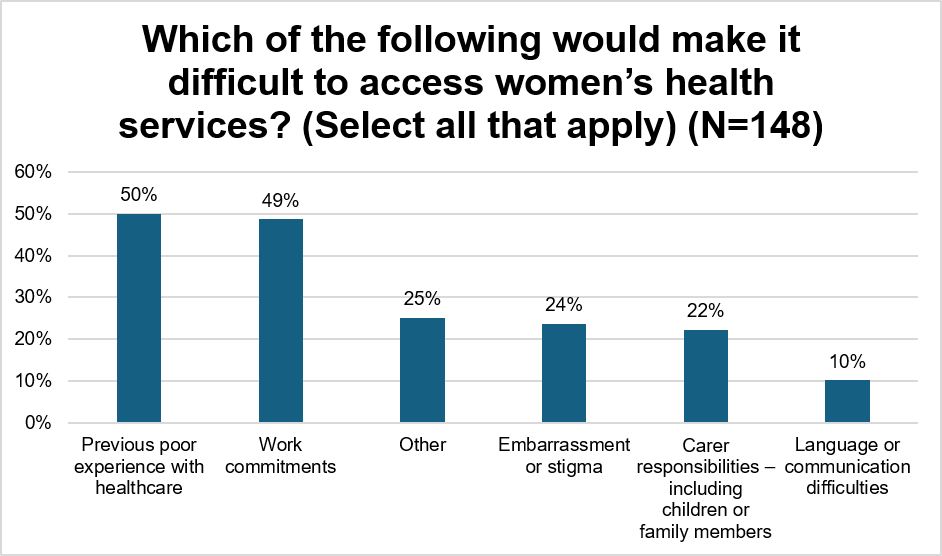
Respondents also shared other barriers that would make it difficult to access women’s health services. These included:
- Transport – not having access to a car or being near bus stops or train stations.
- Location of the clinic and whether there was parking
- Mobility difficulties and not being able to access disabled parking
- Language around gender – “women’s health can make me feel uncomfortable and unwelcome – it makes me expect to be discriminated against”
For those waiting long periods of time for an appointment, having clear information on waiting times, advice on managing symptoms, having a named contact if symptoms change and knowing that a specialist has reviewed their case are the top choices for people.
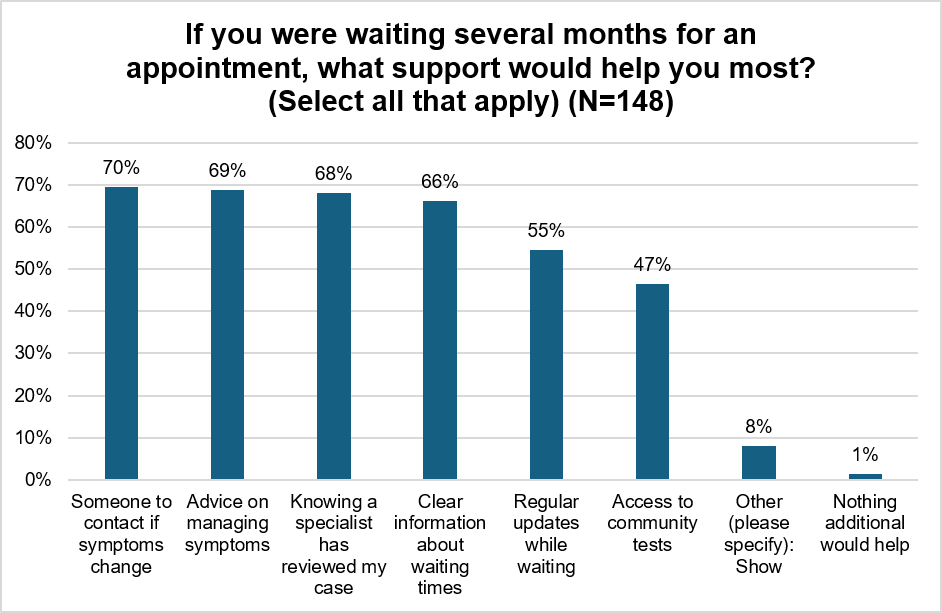
When asked what else would support someone who was on the waiting list, they said
- Being able to check whether symptoms are changing. People want access to tests or monitoring, so they know if their condition is worsening. “Being able to test if symptoms have actually medically changed.”
- Clear guidance on what to do while waiting. Respondents want practical advice, especially if symptoms deteriorate or become unsafe. “Clear guidance on what to do while waiting, especially if symptoms worsen.”
- Confidence that at least one GP has specialist menopause knowledge. Women want reassurance that someone in the practice has proper, up‑to‑date expertise. “Knowing at least one GP in the practice had specific menopause training.”
- Support with employment and daily functioning. Long waits can affect people’s ability to work and live normally. “Paperwork to supply to employer on why I’m in too much pain… to get into my office anymore.”
- The option to attend another clinic. People want flexibility to move their care if waits are too long. “Option to go to another clinic.”
- Emotional and peer support during long waits. Women described loneliness, fear and declining mental health when left without support. “It’s lonely being sick… I needed women going through what I was to make me feel like I wasn’t mad.”
- Honest information about private alternatives. Some want clear guidance about private options when NHS waits are too long. “Advice on how to access private alternatives… my wait was at least 10 months.”
- Ability to move up the waiting list if health deteriorates. People want a fair, transparent way to escalate their care. “Moving up the waiting list if health deteriorated.”
- Transparency about costs if choosing to self‑fund. Some feel forced to consider paying privately and want clarity. “How much I would need to pay to speed things up and potentially save my life!”
- Clear information on switching Trusts without losing waiting time. People want to know how to move to a faster provider without starting again. “No one knows how to request this without losing the accrued waiting time… which is really unfair.”
- Urgent care for severe symptoms, especially heavy bleeding. Some respondents challenge the premise of waiting at all for serious symptoms. “We shouldn’t be waiting months whilst haemorrhaging blood.”
- Regularly reviewed pain management. People want ongoing specialist oversight, not to be left in unmanaged pain. “I’ve been waiting years – still not adequately managed.”
Fairness and Prioritisation
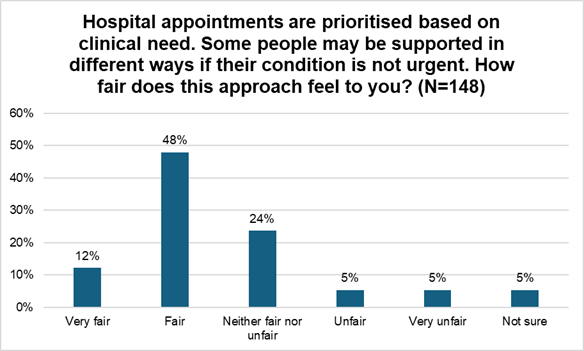
When asked what would help them feel confident that this approach is fair, people said
- Fairness must account for trauma, mental health and life circumstances. People want a system that recognises the impact of trauma, Adverse Childhood Experiences, chronic pain, mental health decline, and the wider pressures women face. “The approach sounds fair but does not take people’s mental health into account.”
- Equalities matter, age, gender, communication and bias. Respondents fear being deprioritised because of who they are, how they communicate, or how their symptoms are perceived. “Being assured that I can trust the system not to marginalise me as a woman over 70.”
- Concern that articulate patients may be prioritised over those who struggle to describe symptoms. People worry the system rewards confidence, not need. “Not everyone is good at describing their conditions and may lead to more articulate being seen quicker.”
- Pregnancy, fertility and time‑sensitive conditions must be recognised Delays can have irreversible consequences for those trying to conceive or experiencing pregnancy loss. “I’ve had painful periods my whole life and now 3 failed pregnancies… timing is crucial.”
- Clear, consistent communication and transparency. People want honest updates about waiting times, decisions, and what to expect. “Radio silence when waiting is awful… there needs to be a system that says where you stand on the list.”
- A fair, understandable and safe prioritisation process. Respondents want to know how urgency is assessed, who decides, and that decisions are based on full information not assumptions or time pressures. “It’s not clear how the assessment is made. Who gets to decide and what criteria are they using?”
- Recognition that ‘non‑urgent’ does not mean ‘not serious’. People want fairness to reflect quality of life, not just clinical risk. “Even if a condition is not considered urgent, it can still have a significant impact on daily life.”
- Ability to escalate if symptoms worsen. Fairness means having a clear route to move up the list when health deteriorates. “That there is a system for moving up the waiting list if condition changes.”
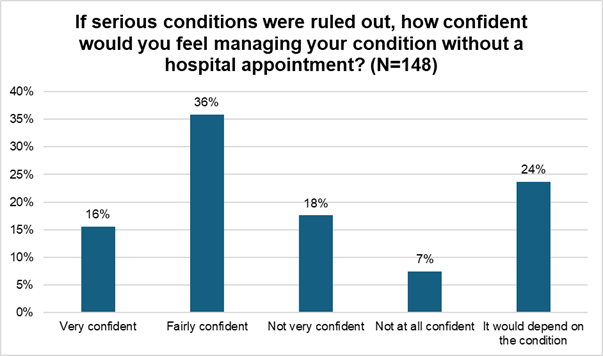
- Proper diagnostics and early rule‑out of serious conditions. People want reassurance that serious issues are checked for early, and that delays won’t cause harm. “Knowing that serious conditions were ruled out before being referred for an appointment in a few months’ time.
- Access to advice, support and interim care while waiting. Fairness includes having someone to talk to, symptom management, and emotional support. “A chance to talk with a health care professional.
- Joined‑up records and consistent documentation People want confidence that everyone involved can see their history and decisions are based on accurate information. “A shared system that all staff can access to view and update patient notes.”
What else could we consider?
When asked what else they would like us to consider about women’s health services, people said…
- Equalities, inclusion and cultural safety must be central. Women want services that recognise cultural, religious, linguistic and socioeconomic needs — and ensure everyone feels welcome, safe and respected. “Ensure services are accessible and inclusive for all women, including those from diverse cultural, language, and socioeconomic backgrounds.”
- Trauma‑informed care is essential. Many respondents described trauma, difficult past experiences, and the need for services that understand and respond sensitively. “Learn about the impact of trauma and apply the knowledge. Take our pain seriously.”
- Respect, dignity and being believed. Women want to be listened to, not dismissed, patronised or minimised, especially during intimate examinations. “Stop treating us like we are panicking or exaggerating… listen to us.”
- Gender‑sensitive care and choice of practitioner. Some women emphasised the importance of female clinicians for intimate care, and of services designed around women’s needs.“Ensuring cultural and religious needs are met… female practitioners offered.”
- Endometriosis and chronic gynaecological conditions must be taken seriously
Women repeatedly described years of pain, dismissal and lack of specialist expertise.“Please start training doctors and physios specifically in endometriosis… that is the only treatment.”
- Accessibility, appointments, location, flexibility. Women want services that are easy to reach, with evening/weekend appointments and drop‑in options.“Make it easier to attend appointments by offering evening and Saturday appointments.”
- Pain relief and humane treatment during procedures. Many described painful, distressing experiences during examinations and want better pain management.“We need more pain relief than ‘soon be over’.”
- Stop blaming weight, stop assuming fertility, treat women as individuals. Women want personalised care, not stereotypes or assumptions. “Don’t assume that all women want kids… consider real women’s lives and symptoms.”
- Education and awareness for women and girls. Respondents want better public understanding of women’s health, hormones, contraception and symptoms.“Health education for women and girls, so they know when to seek advice.”
- Inclusion, safety and language. A small number of respondents raised concerns about privacy and safety in women‑only spaces, particularly during intimate care or inpatient stays. These views were strongly expressed but represented a minority of responses. At the same time, other respondents felt that women’s health services should avoid over‑gendered language, noting that this can make some people feel excluded or unwelcome.
- Bringing in our community and voluntary sector to support people. People found support in the community and voluntary sector and found this to be important in raising awareness, peer support and knowing how to advocate for themselves.
Conclusion
People want improvements to women’s health services. They would like better menopause care and GPs with training to diagnose and treat common and complex conditions correctly. Getting faster access to tests and scans is crucial as any delay could lead to missed diagnoses.
Women also stressed that procedures need to be handled sensitively and with adequate pain relief, since many find them distressing. Care needs to be joined up properly, with better communication between GPs, community services and hospitals rather than patients having to navigate these separately. The services need more funding and staff to cope with demand and reduce waiting times.
Beyond clinical care, women and girls need better information about their bodies and symptoms so they know when to seek help. And fundamentally, women need to be listened to and believed. Too many felt dismissed or not taken seriously, and that’s stopping people from getting the care they need.