Overview
A total of 187 people completed the gastroenterology outpatients survey, which ran from 20 March to 20 April 2026.
We ran this survey to understand people’s experiences, expectations and views of gastroenterology services, to help inform how care for digestive symptoms can be improved across south west London. The focus was on how people move through the pathway, from first seeking help in primary care or community settings, through to referral, diagnosis and specialist treatment and whether care is being delivered in the right place, at the right time, with the right support.
Gastroenterology services support a wide range of digestive conditions, including abdominal pain, changes in bowel habits, reflux, IBS and inflammatory bowel disease. People may be assessed and managed in different settings, including GP practices, community services and hospital outpatient clinics, depending on clinical need.
Most people who responded to the survey had sought help through their GP practice (42%)or a hospital specialist (14%) or in multiple health care settings (24%). 13% who completed the survey had not sought help for their digestive issue.
Overall, findings showed mixed experiences. While some people described positive and supportive care, some reported delays, difficulty accessing appointments, inconsistent communication and concerns about not feeling listened to or believed.
Methodology
We developed these surveys with ICB clinical leads and Acute Provider Collaborative colleagues, to better understand people’s experiences of gastroenterology conditions and care. It was widely shared through partner organisations, including voluntary and community sector networks, who distributed it within their local communities. It was also promoted through paid for adverts across organisational social media channels to reach people with experience of digestive symptoms and outpatient care across South West London.
The survey was open to adults who had used outpatient services in the past two years or who may need to use them in future.
As with all open surveys, findings are not representative of the wider population and reflect the views of those who chose to respond. The sample is self-selecting and likely to be influenced by individuals with stronger experiences or interest in the topic.
The survey had a higher proportion of older adults and people identifying as White British/White English, meaning some communities may be under-represented.
Responses were also gathered online, which may have created barriers for some groups, particularly those with limited digital access or lower health literacy.The survey was open to adults who had used outpatient services in the past two years or who may need to use them in future.
As with all open surveys, findings are not representative of the wider population and reflect the views of those who chose to respond. The sample is self-selecting and likely to be influenced by individuals with stronger experiences or interest in the topic.
The survey had a higher proportion of older adults and people identifying as White British/White English, meaning some communities may be under-represented.
Responses were also gathered online, which may have created barriers for some groups, particularly those with limited digital access or lower health literacy.
The survey was open to adults who had used outpatient services in the past two years or who may need to use them in future.
As with all open surveys, findings are not representative of the wider population and reflect the views of those who chose to respond. The sample is self-selecting and likely to be influenced by individuals with stronger experiences or interest in the topic.
The survey had a higher proportion of older adults and people identifying as White British/White English, meaning some communities may be under-represented.
Responses were also gathered online, which may have created barriers for some groups, particularly those with limited digital access or lower health literacy.
Summary of key findings
- Long waits and delayed follow-up are leaving people without reassurance or support. People described long waits for appointments, tests, results and follow-up care. Many felt abandoned once serious conditions had been ruled out, despite ongoing symptoms which continued to impact on daily life.
- Communication and coordination across services need to improve. People frequently reported poor communication about referrals, appointments, results and next steps. Many people said they had to chase services themselves and wanted more regular updates, clearer information and better joined up working between GP practices, hospitals and specialist teams.
- People want to feel listened to and taken seriously
A strong theme throughout the survey was frustration at symptoms being dismissed, minimised or managed through generic pathways. People wanted more personalised, holistic care that considered their wider health, lived experience and quality of life. - Access to timely specialist investigation and expertise is highly valued
Many people described positive experiences when they were able to access timely tests, specialist review and investigations, particularly where symptoms suggested a serious condition. Respondents valued having serious conditions ruled out quickly and felt reassured when they received prompt referrals, diagnostic tests and clear clinical advice. However, delays in accessing diagnostics, gastroenterology appointments and specialist expertise remained a consistent concern. - Digestive conditions and delays in care are affecting people’s mental wellbeing
Many people described anxiety, stress and uncertainty caused by ongoing symptoms, lack of answers and long waiting periods. Some people said they felt forgotten within the system, while others highlighted the wider impact on confidence, work and everyday life.
Summary in response to key questions
- Initial access to care: Most people first sought help through their GP (42%), with experiences ranging from fast referrals and supportive care to delays, limited communication and difficulty accessing follow-up support.
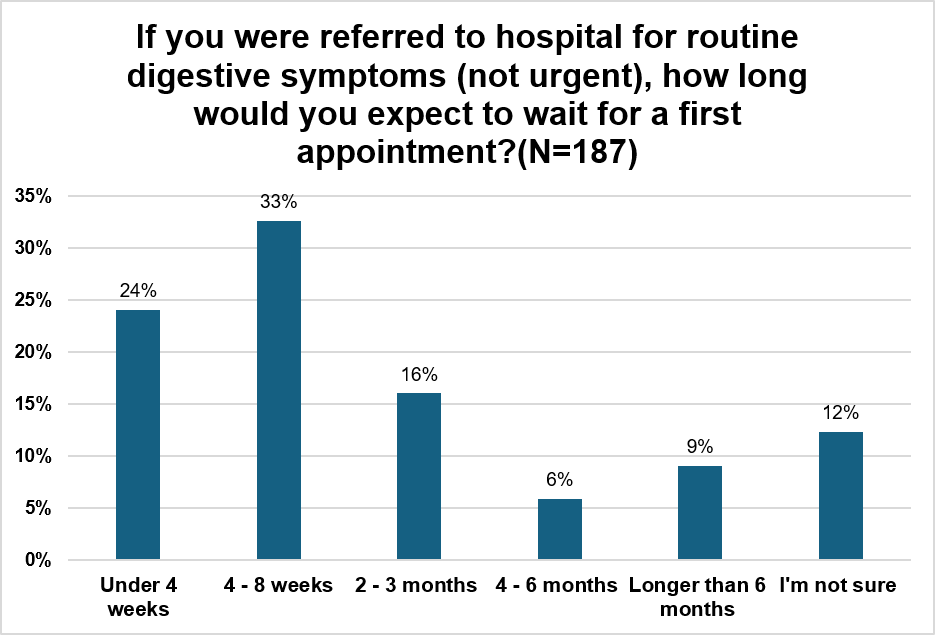
- Waiting times: People generally felt that when symptoms suggested a potentially serious condition, they were investigated quickly. Many described prompt GP referrals, particularly through urgent cancer pathways, with rapid access to colonoscopies, endoscopies, scans and specialist tests. Several respondents valued the speed with which serious conditions could be ruled out, providing reassurance even when a diagnosis was not immediately found. However, this contrasted with experiences of routine referrals, where many people reported waiting several months to over a year to see a specialist. When waiting for an appointment, people would like someone to contact if symptoms worsen, advice on managing symptoms and updates on waiting times.
- Fairness and prioritisation: Most respondents (nearly 60%) felt it was fair to prioritise patients according to clinical need, recognising that those with the greatest need should be seen first. People generally supported clinical prioritisation but wanted transparency about how decisions are made, reassurance that criteria are applied consistently, and mechanisms to review priority if symptoms worsen while waiting.
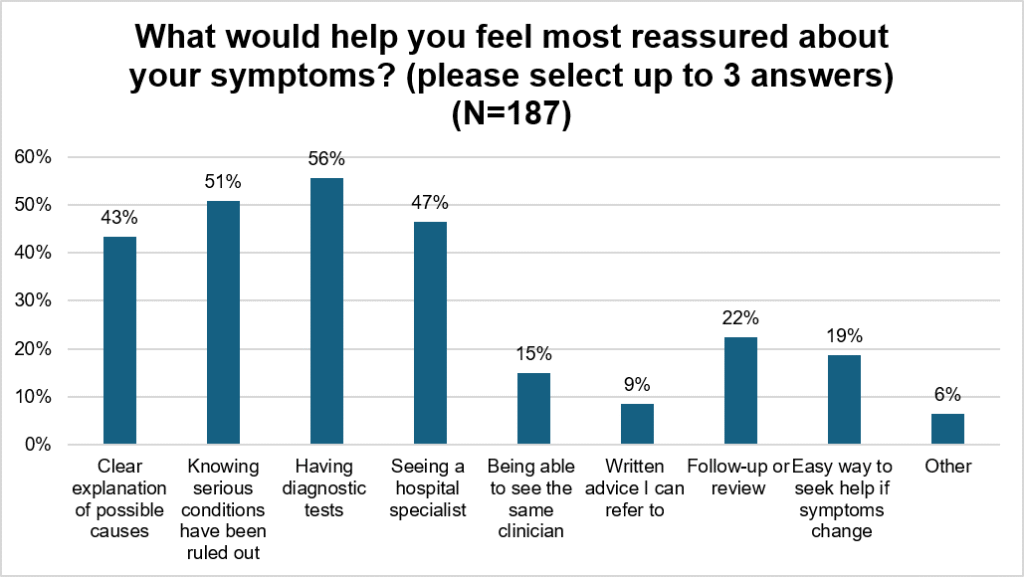
- Reassurance and communication: When asked what people would find reassuring, Confidence increased when tests were quick, results were clearly explained and clinicians provided reassurance that serious conditions had been ruled out. Anxiety was often linked to ongoing symptoms, uncertainty, a lack of updates and living with a condition for long periods of time with limited support.
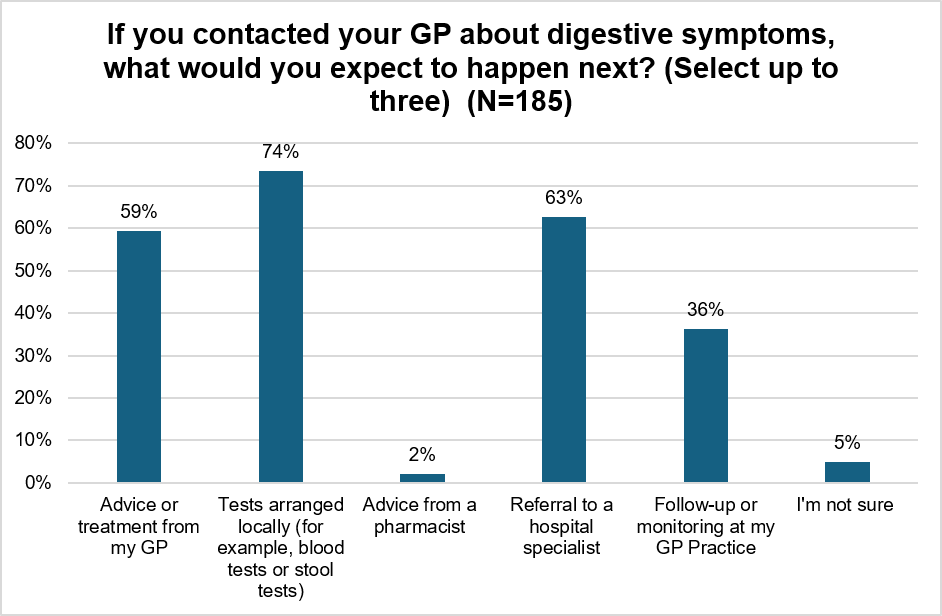
- Expectations of care: People expected action from services, including advice, investigations, monitoring and referral to specialists where needed, alongside clearer information and better coordination between GP, Community and Hospital services.
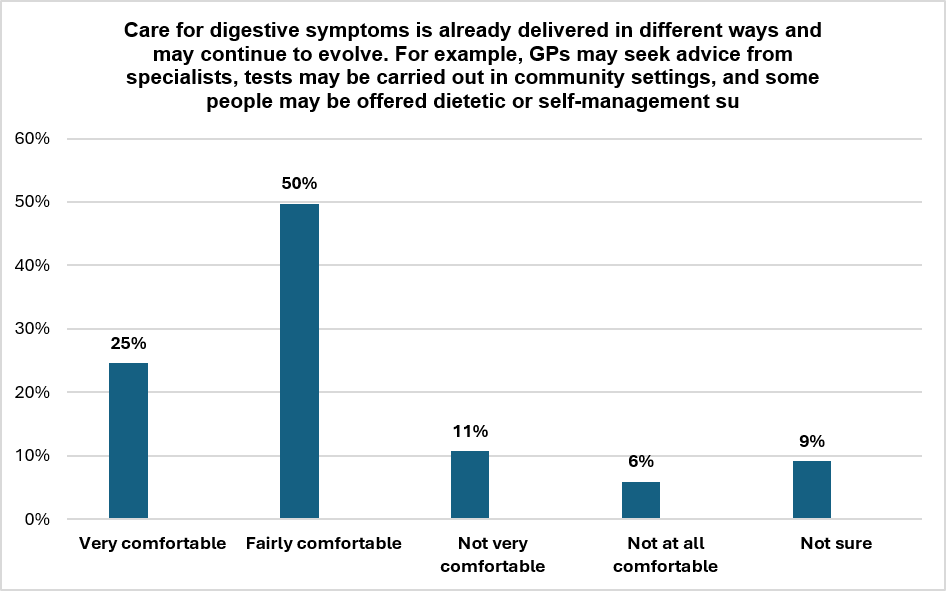
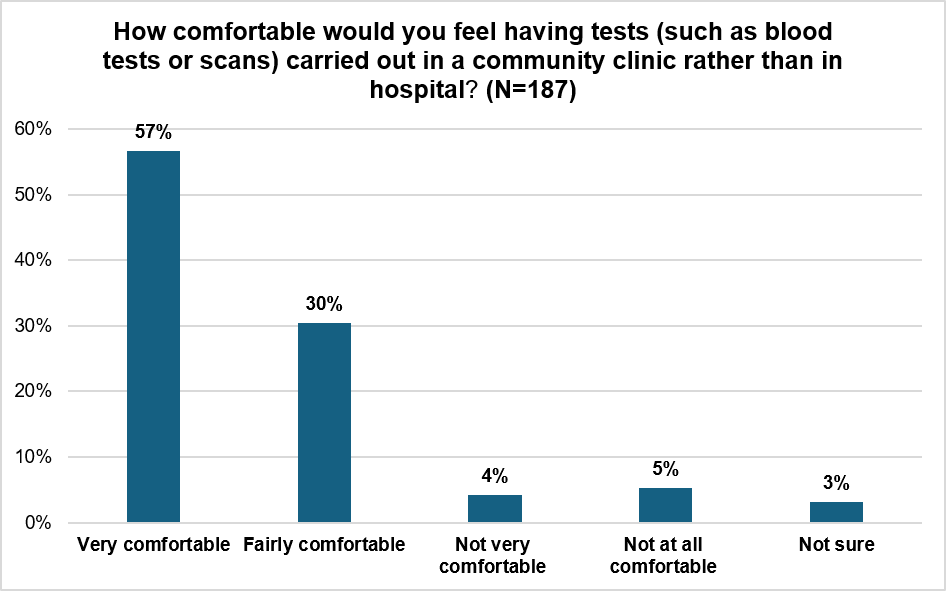
- Views on community-based care: Many were open to local or GP led specialist input and non-hospital testing, particularly for stable conditions or where serious illness had been excluded, but confidence decreased when symptoms were severe, persistent or unexplained. People wanted reassurance they would still have access to specialist gastroenterology expertise when needed.
- Group and alternative models: Views were mixed on group consultations, with some valuing shared support and quicker access, while others preferred individual appointments due to privacy concerns, if conditions were complex and cultural barriers.
- Overall suggestions for improvement: People would like better communication, continuity of care, timely updates and clear clinical oversight. This would be key to improving confidence in more flexible gastroenterology pathways.
Who we heard from
This section explores who responded to our survey. As these questions were not mandatory, a significant number of people skipped some or all of them. As a result, the findings may not fully reflect the characteristics of the whole sample.
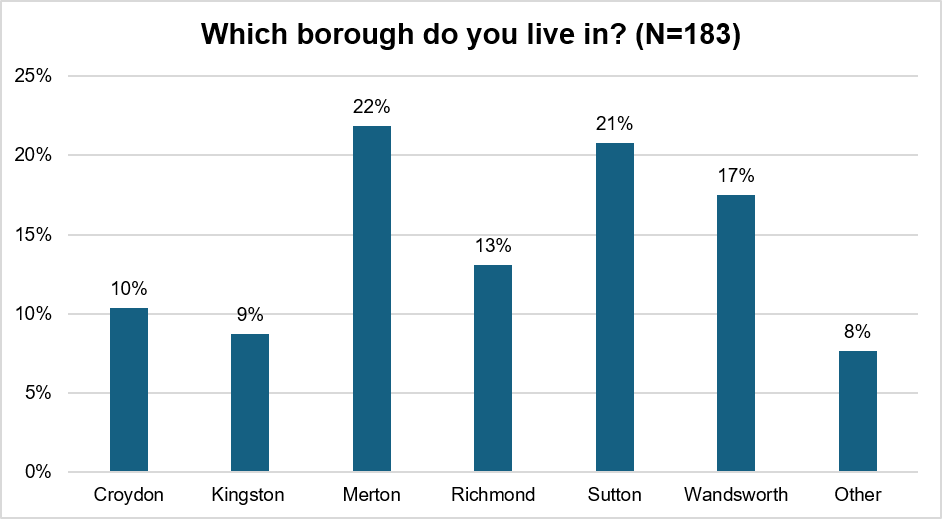
Borough (183 out of 187 responses)
When asked which borough they live in, responses showed that Merton was the most represented of our six south west London boroughs with 22% of respondents, followed closely by Sutton at 21%. Wandsworth had 17% of responses, Richmond 13%, Croydon 10%, Kingston 9%, with 8% selecting other areas which included Lambeth and Surrey.
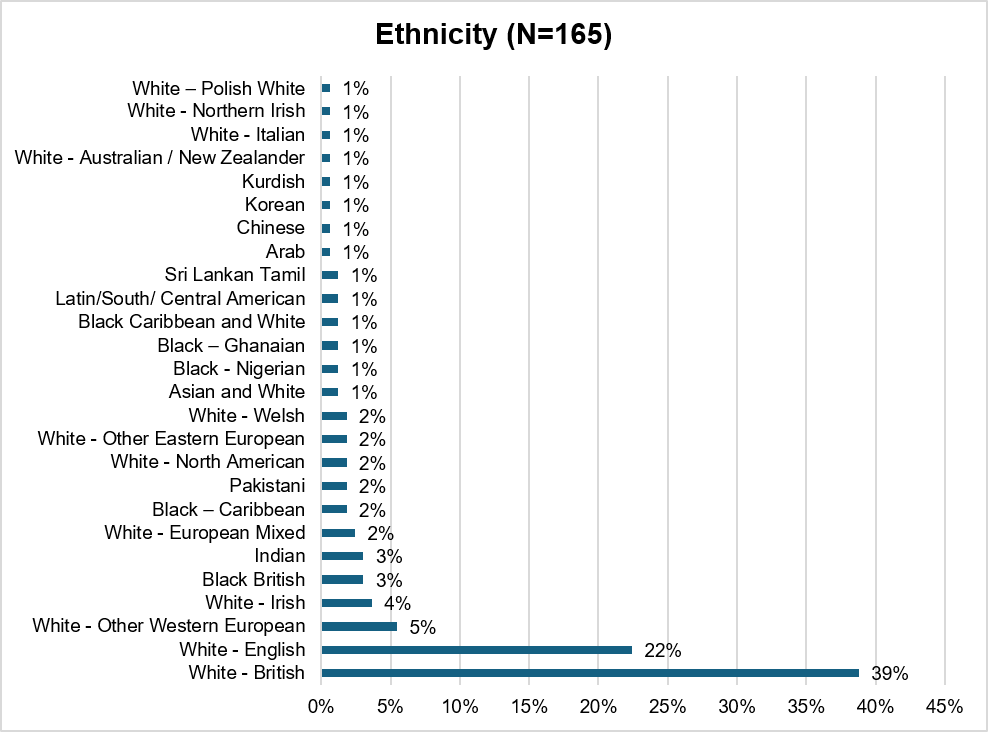
Ethnicity (165 out of 187 responses)
Most people completing this survey identified as White British or White English, making up 39% and 22% of responses. A further 5% identified as White Other Western European, and 4% as White Irish.
Black British and Indian respondents each made up 3% of responses. Several other groups were represented at smaller levels: White European Mixed, Black Caribbean, Pakistani, White North American, White Other Eastern European, and White Welsh respondents each accounted for 2% of responses.
A range of other ethnic backgrounds were also represented, including Asian and White, Black Nigerian, Black Ghanaian, Black Caribbean and White, Latin/South/Central American, Sri Lankan Tamil, Arab, Chinese, Korean, Kurdish, White Australian/New Zealander, White Italian, White Northern Irish, and White Polish. Each of these groups made up 1% of responses.
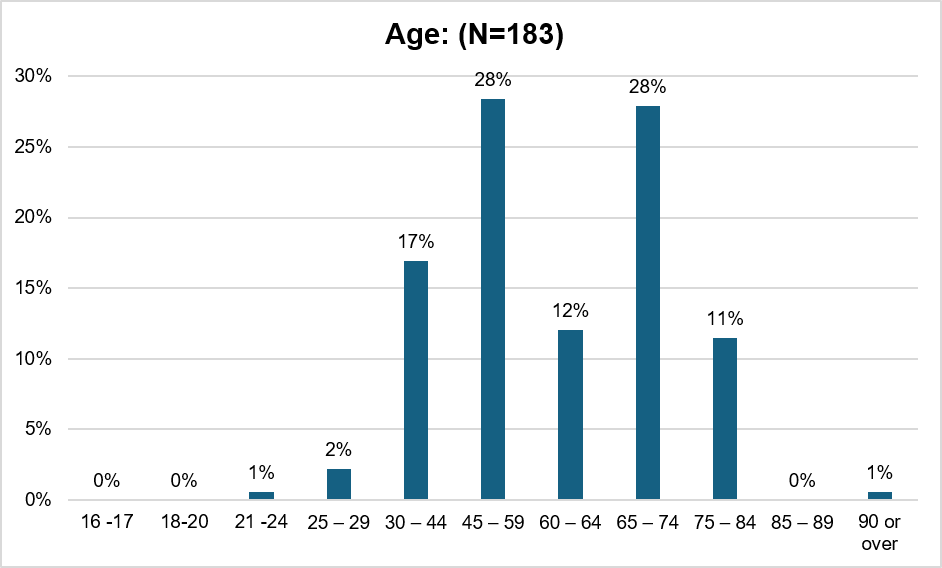
Age (183 out of 187 responses)
Responses revealed an older demographic overall. No respondents were aged 16-20, and only 1% were aged 21-24. The 25-29 age group represented 2%, while the 30-44 age group made up 17%. The largest groups were aged 45-59 (28%) and 65-74 (28%). The 60-64 age group represented 12%, with 75-84 year-olds accounting for 11%. Only 1% of respondents were 90 or over, and none were 85-89.
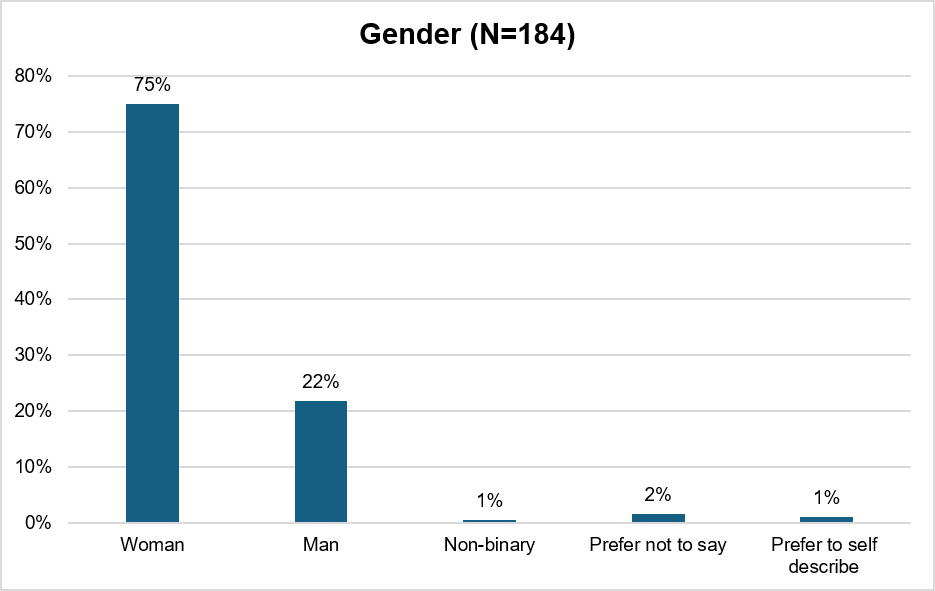
Gender (184 out of 187 responses)
Responses showed the survey was predominantly female, with women making up 75% of respondents. Men accounted for 22% of responses. Non-binary respondents represented 1%, those preferring not to say made up 2%, and those preferring to self-describe represented 1%.
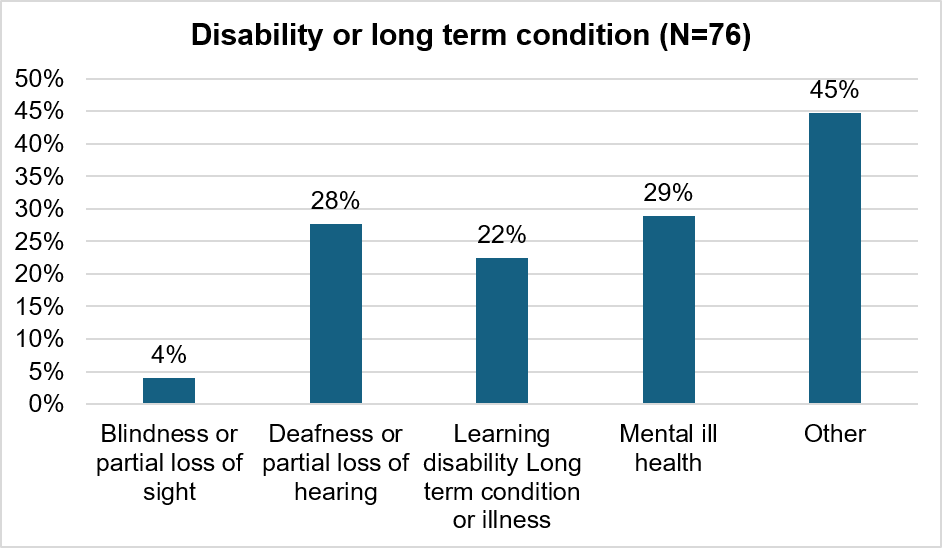
Disability or Long-term Condition (76 out of 187 responses)
When respondents disclosed disability or long-term conditions, 45% indicated “other” conditions not specified in the categories. Mental ill health was reported by 29% of those who answered this question, while 28% reported deafness or partial loss of hearing. Learning disability or long-term condition/illness was reported by 22%, and blindness or partial loss of sight by 4%.
Carers (180 out of 187 responses)
Responses indicated that 80% of respondents are not carers, while 20% reported having caring responsibilities for someone else.
Experiences of accessing support and care for digestive issues
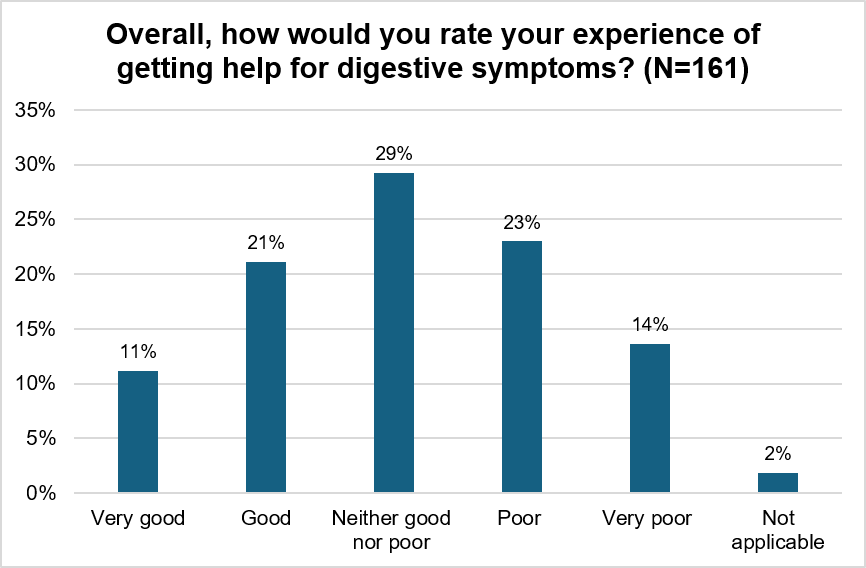
161 people rated their experience of help and support for digestive symptoms. Overall, the findings show variation in experiences, with several people reporting challenges in getting support for digestive symptoms.
Around a third of respondents rated their care as good or very good. Positive experiences were often linked to being listened to, receiving prompt referrals and investigations, and having serious conditions ruled out quickly. However, experiences were mixed overall, with over a third reporting poor experiences, largely driven by lengthy waits for specialist care and limited support while waiting for appointments.
What has worked well?
People valued being listened to, taken seriously and referred for tests quickly. Many People said the most positive part of their experience was when GPs or specialists listened carefully to their symptoms, acted quickly and arranged further tests. People appreciated prompt referrals for colonoscopies, endoscopies, scans and blood or stool tests, particularly where serious conditions needed to be ruled out. A number of responses described positive experiences where cancer pathways or urgent referrals moved quickly, helping them feel reassured. Others valued clinicians who spent time understanding symptoms.
“Dr J spent time with me to ask questions and find the cause of my issues.”
Medication, dietary changes and symptom management helped some people manage their condition. Several people said prescribed medication had relieved symptoms or helped control flare-ups, while others found dietary changes useful. People mentioned low FODMAP advice, lactose-free diets and supplements as helpful in managing symptoms.
“The prescribed medication has helped when my symptoms occur.”
Positive experiences when staff take the time to listen and provide excellent care. People frequently highlighted caring, proactive or supportive clinicians as making the biggest difference to their experience. People valued staff who took time to explain conditions, investigate symptoms thoroughly and provide reassurance. IBD nurses were also mentioned positively.
“I have access to specialist IBD nurses who are available via email.”
People felt urgent or ‘red flag’ symptoms were generally responded to more quickly. People who reported symptoms associated with possible cancer or serious illness often described fast referrals and investigations.
“If you have red flags, you are investigated quickly”
What could be improved?
Long waiting times, delays and repeated appointment cancellations cause frustration. Many people described lengthy waits for consultant appointments, diagnostic tests, scans and follow-up care. People said appointments were regularly cancelled, postponed or delayed, sometimes multiple times, leaving them without reassurance, treatment or ongoing support while symptoms continued or worsened. Some people described waiting months or more than a year for appointments or investigations, including ultrasounds, colonoscopies, MRI scans and specialist gastroenterology support. Some felt delays meant conditions could worsen before they were investigated, particularly where digestive conditions fluctuate over time.
“Inflammatory bowel disease is a fluctuating condition and for the problems to be seen, the tests need to happen when the flare up is happening and not over a year after referral.”
People want better communication, clearer updates and more joined-up care across services. People described poor communication about appointments, referrals, investigation results and next steps. Many said they had to repeatedly chase hospitals or GP surgeries themselves for updates, while others described confusion caused by multiple communication systems, missing letters or inconsistent advice between professionals. Several people also highlighted poor coordination between departments and services, particularly where digestive symptoms overlapped with gynaecology, mental health or other long-term conditions.
“There is no holistic approach. Gastroenterologists know nothing about endometriosis or adenomyosis.”
People want quicker access to specialist care, investigations and follow-up support. People described delays in accessing consultants, specialist nurses and diagnostic tests, particularly where symptoms were ongoing but not considered urgent. People often felt they were left waiting without support after initial tests ruled out cancer or other serious conditions. Several people wanted quicker access to endoscopy, scans, SIBO testing and gastroenterology appointments. A few responses raised concerns that timely access could depended on whether people could afford private healthcare.
“I had no other option than to go to a private practice and subsequently pay for the consultation and test myself.”
People wanted to feel listened to, believed and treated as individuals rather than being dismissed. A strong theme throughout responses was frustration at not feeling heard or taken seriously by healthcare professionals. Some people felt symptoms were minimised, attributed to anxiety, age, alcohol use or gender, or managed with repeat prescriptions rather than proper investigation. Others felt clinicians relied too heavily on generic pathways or “tick box” assessments rather than understanding individual circumstances, symptoms and family history.
“Focus on the patient, the symptoms/problem and their needs rather than trying to quickly get through the process and ticking boxes.”
People wanted more personalised and preventative support rather than medication-focused care alone. Many people felt care focused heavily on prescribing medication without enough discussion about diet, nutrition, lifestyle changes, symptom management or underlying causes. People wanted better access to dietitians, nutritionists, specialist nurses and practical advice while waiting for investigations. Some people also wanted greater monitoring and earlier intervention to prevent conditions worsening.
“We need individual help with a good food plan that takes our problems into account.”
There were concerns about knowledge and understanding of digestive conditions within primary care and wider services. Several people felt there was limited understanding of conditions such as irritable bowel syndrome (IBS), Small Intestinal Bacterial Overgrowth (SIBO), reflux, microbiome-related issues and complex digestive disorders. People described being repeatedly prescribed medication without clear diagnoses or discussion of alternatives. Others felt clinicians lacked awareness of how digestive symptoms intersect with women’s health, neurodiversity, trauma or mental health needs.
“Have more understanding of people with autism and other mental health issues when it comes to the hospital part of the service.”
Mental health, anxiety and the emotional impact of digestive conditions were raised throughout responses. Many people described the stress and uncertainty caused by long waits, ongoing symptoms and lack of answers. Some people said they were left frightened about possible cancer or worsening conditions while waiting for appointments. Others described the impact on confidence, work, relationships and quality of life.
Some responses also described traumatic experiences during investigations or hospital stays, particularly where emotional needs were not considered alongside physical care. One parent explained how their daughter’s mental health needs and fear of procedures were not appropriately supported during a colonoscopy appointment.
Some people said gaps in digestive care led them to use A&E or emergency services instead. Several people described turning to A&E because they could not access timely outpatient or specialist care, or because symptoms worsened while waiting for investigations. Others felt emergency care pathways were quicker than planned care routes.
“Next time… I will go to A and E instead in the hope I am seen there. Thereby adding to pressures on A and E.”
Follow-up care and ongoing support were often described as inconsistent or lacking altogether. Some people said that once serious illness had been ruled out, they felt left alone to manage ongoing symptoms. People described a lack of follow-up appointments, poor continuity of care and limited practical support after diagnosis. Several people also worried about monitoring for long-term conditions or cancer risk because follow-up appointments had stopped or been delayed. Some People also raised concerns about dignity, preparation and information before procedures, including inadequate information about colonoscopies and FIT testing.
“Once you are cleared of having a life-threatening illness you are left completely on your own with no help.”
Administrative problems and barriers to accessing care added further frustration for people. People described problems booking GP appointments, difficulties contacting outpatient departments and concerns about lost referrals, missing forms and delayed letters. Others raised concerns about appointment systems moving from face-to-face to telephone appointments, or communication being spread across letters, texts, apps and emails.
“Admin! Inefficient and unable to access them by phone.”
Experience of Urgent and Emergency Care for digestive issues
This section explores people’s experiences of urgent and emergency care for digestive symptoms and what could have been done earlier or differently to support people to seek the right care, in the right setting.
91% of people had not been to A&E or urgent care because of digestive symptoms. 8% of people had and 1% were not sure.
When asked what could have been done earlier or differently to receive care in a more appropriate setting, people said:
- Prevention measures could have been taken more seriously. They felt their symptoms hadn’t been fully investigated previously, leading to a deterioration in their condition.
- Difficulty accessing GP appointments. People felt that delays in accessing primary care sometimes prevented them from getting advice, assessment or treatment early enough. Some said this led them to seek help through A&E when their symptoms worsened or when they felt they had no other option.
- Poor continuity of care and lack of follow-up after emergency treatment. Several people described being discharged from A&E or hospital without clear aftercare, follow-up appointments or ongoing management plans
Expectations and reassurance
This section explores people’s expectations around waiting times, investigations and follow-up care for digestive symptoms. It looks at what people consider a reasonable timeframe for a routine appointment and what support they expect after contacting their GP.
It also highlights the types of care and investigation people assume will be offered, including access to tests, specialist referral and ongoing monitoring in primary care.
Finally, it outlines what most helps people feel reassured while waiting, which had a strong preference quick investigations, clear communication and confidence that symptoms are being properly assessed and followed up.
Exploring new ways of delivering care
This section explores people’s expectations of digestive symptom care and the level of reassurance they need when care is delivered in different ways. It looks at how comfortable people feel with more flexible and community-based approaches, including group consultations, community testing and support outside of hospital settings.
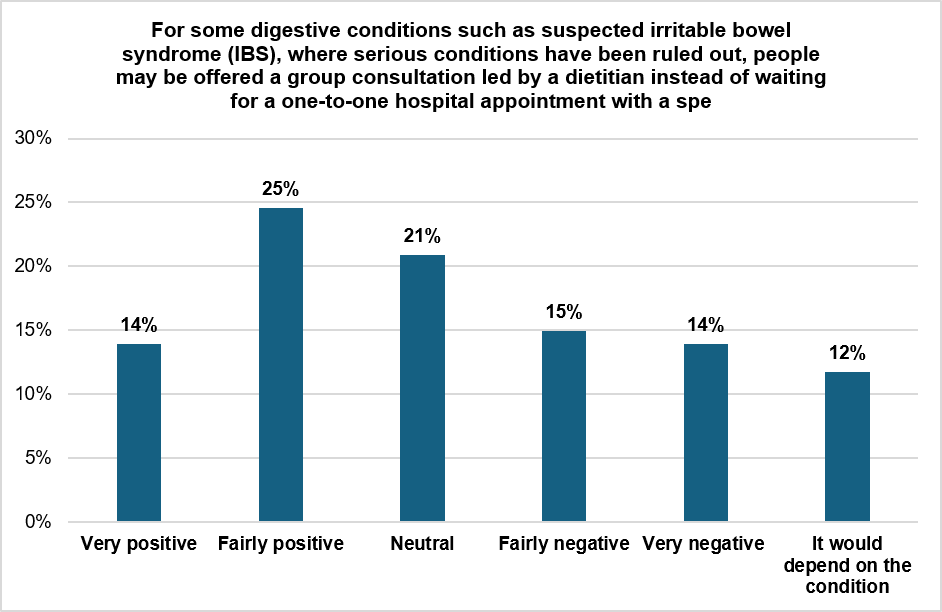
When asked what would make this type of group support would feel helpful and appropriate, people said:
Group support should be small, targeted, and well facilitated. Where people were open to group support, they said it would need to feel targeted, practical, and inclusive. People said they preferred having the option to talk in smaller groups, support focused on specific conditions or symptoms and opportunities to ask questions privately if needed. People also highlighted the importance of skilled facilitators, clear information, flexible formats, and accessible support.
“Groups should be welcoming, inclusive, and tailored to participants’ needs. Information should not feel “one size fits all.”
Group support could provide reassurance, advice and quicker access to support. Some felt group support could help those feel less alone and provide opportunities to learn from others with similar symptoms or conditions. People valued hearing “how others manage their conditions”, sharing practical advice, and learning from “other people’s stories.”Several people also felt group support could provide quicker access to advice and support while waiting for specialist appointments.
“I would feel like I’m getting some support while waiting for a hospital appointment.”
People were more positive about groups when they involved professional input, particularly from dietitians or clinicians. People said support would feel more appropriate with “the presence of a medical practitioner” or “a qualified practitioner.”
Group support had mechanisms in place to protect privacy, embarrassment and any discomfort. Many people said they would feel uncomfortable discussing digestive symptoms in a group setting because the issues felt too personal or embarrassing.
“I don’t want to discuss private issues within a group. I would absolutely not want to describe personal issues with a group of strangers.”
Confidentiality and privacy were also important concerns, particularly for neurodivergent people and those with complex health conditions.
“Groups are generally not my thing being autistic.”
Several people said they would prefer one-to-one support, online resources, or written information instead of group sessions.
Group support does not replace specialist care. A strong theme throughout responses was concern that digestive symptoms are highly individual and should not be managed through generic advice alone.
“Every patient is different in terms of symptoms,”
Many people said group support would only feel appropriate after serious conditions had been ruled out or after receiving a clear diagnosis.
“If I already felt confident that the right tests had been done and serious conditions ruled out”
People also stressed that group support should not replace one-to-one or specialist care.
“It should not though be instead of individual discussion and assessment”
When asked what concerns people had about these different approaches, they said:
Information accuracy and communication risks. Concerns were raised about the accuracy of information being captured, interpreted, and shared between services. Some felt there is a risk that key details could be misunderstood, not correctly recorded, or lost during referral or handover processes, leading to inappropriate advice or decisions.
Risk of missing something serious or incorrect diagnosis. A concern was that important symptoms or underlying conditions could be missed. People worried that remote assessment, group approaches, or reduced specialist contact could lead to delayed diagnosis or failure to identify more serious conditions.
Trust, being taken seriously, and clinical judgement. Some people questioned whether their symptoms would be taken seriously, with concerns about being dismissed or not believed. Previous negative experiences shaped expectations, with some expressing low trust in clinical judgement or consistency of care.
“One size fits all” approaches would not reflect individual needs. People highlighted that symptoms can be complex, overlapping, or influenced by multiple conditions, and worried that standard pathways may oversimplify their situation.
Access to follow-up, escalation, and specialist care. People wanted reassurance that there would be clear routes back into specialist care if symptoms worsened or advice did not help. Concerns included being left without ongoing support, or uncertainty about how quickly they could be re-referred.
Delays, waiting times, and reduced access to specialists. Some felt these approaches could slow access to diagnosis or specialist review, potentially extending time to treatment. There was concern that new models could increase waiting times or create barriers to seeing the right clinician.
Preference for face-to-face care and limitations of remote/group models. There were concerns that remote advice, letters, or group consultations may not be suitable for all conditions or individuals. Some felt these formats reduce opportunity for reassurance, personal discussion, or sensitive communication.
System pressures and concerns about cost-cutting. Several responses linked these approaches to wider NHS pressures, including perceptions that changes are driven by resource constraints rather than patient need. There are concerns about the quality of care being reduced.
What support do people want whilst waiting?
This section explores what support would help individuals whilst waiting for an appointment.
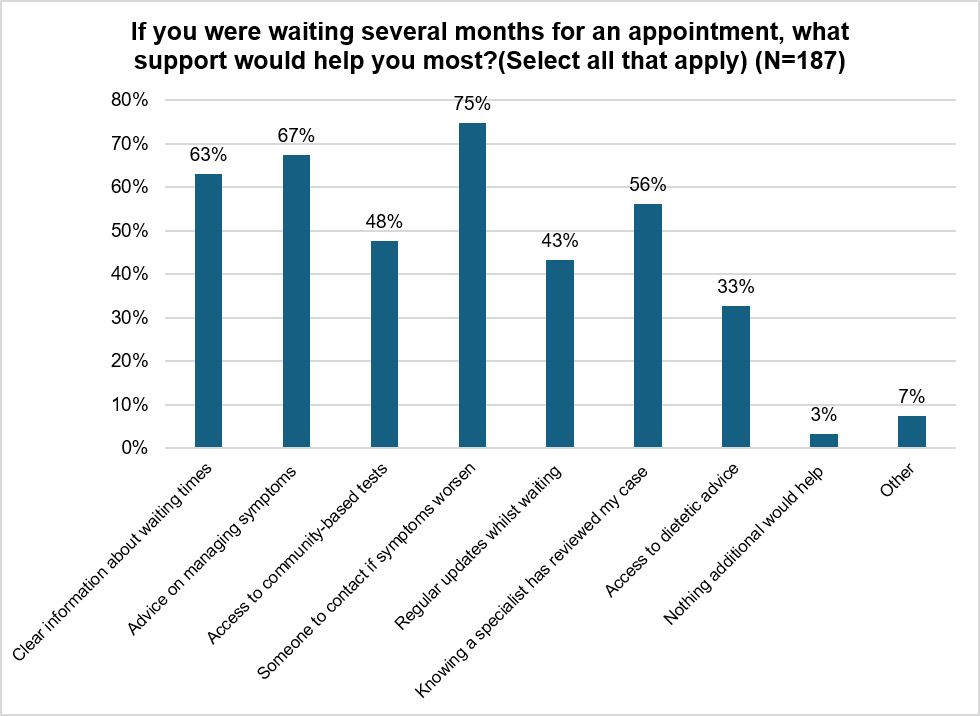
When asked what other things could support people whilst they were on the waiting list, people said:
Clarity on what to do if their condition deteriorates while waiting. This includes access to condition-specific advice, emergency guidance, or clear pathways for urgent support without having to repeatedly re-explain their history through generic services.
Having continuity through the full diagnostic pathway. A concern was that delays should not repeat at multiple stages. People highlighted frustration at waiting again for tests, results, or follow-up appointments after initial delays, with a strong preference for a joined-up process from referral through to diagnosis.
Having regular updates while waiting, and reassurance that they have not been forgotten. Lack of communication was linked to anxiety and uncertainty about whether their case is progressing. People want to have regular updates and reassurance that the NHS hasn’t forgotten about them.
The ability to access support in urgent or changing circumstances. People want practical support options during the waiting period, including access to cancellation slots, sick notes where needed and timely testing when symptoms are active rather than delayed beyond clinical relevance.
Some challenged the question itself, expressing anger and frustration at long waiting times. There was a view that waits of several months are unacceptable and should be reduced to weeks with concern that the system is focusing on managing waits rather than addressing the underlying capacity issues.
A small number raised concerns about financial pressure on services and perceptions of cost-cutting, alongside broader scepticism about whether proposed support options reflect genuine patient need.
Fairness and prioritisation
This section explores views on different ways that people could be supported based on their clinical needs.
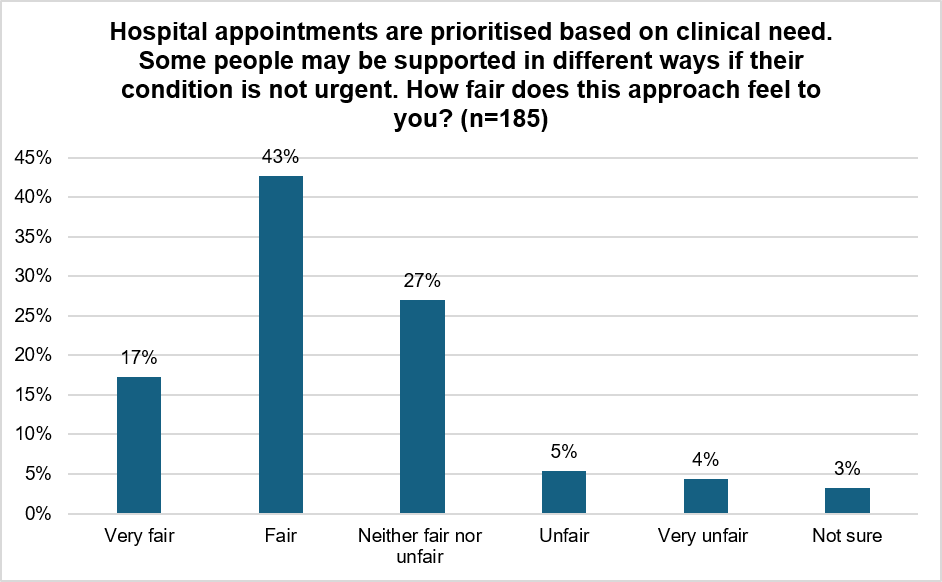
When asked about how they would feel about prioritisation based on clinical need and what would help make it fair, people focused on reassurance, transparency, and trust in how decisions are made. They also highlighted concerns about how urgency is defined, whether symptoms are fully understood, and what happens if conditions change while waiting.
Clear and transparent criteria for prioritisation. People want clarity on how clinical need is assessed and how prioritisation decisions are made. This includes understanding what makes a condition “urgent” and reassurance that criteria are applied consistently and fairly.
Trust in fairness and clinical judgement. A key theme is trust in whether prioritisation decisions are fair and accurate. Some people expressed confidence in clinical triage, while others questioned whether decisions would be made appropriately or consistently across patients.
Concern that symptoms may be underestimated or misclassified. Many worry that symptoms could be wrongly judged as non-urgent, particularly where serious conditions may initially present with mild or non-specific symptoms. There is concern that underestimation could delay diagnosis or lead to deterioration while waiting.
Risk of deterioration while waiting. People highlight that conditions can worsen over time, and that delays may result in patients becoming more unwell while remaining on lower priority pathways. There is concern about patients being “pushed down the list” despite their symptoms changing or needing more urgent treatment.
Need for regular updates and communication. People want ongoing communication about waiting list status and progress. Being kept informed is seen as essential to
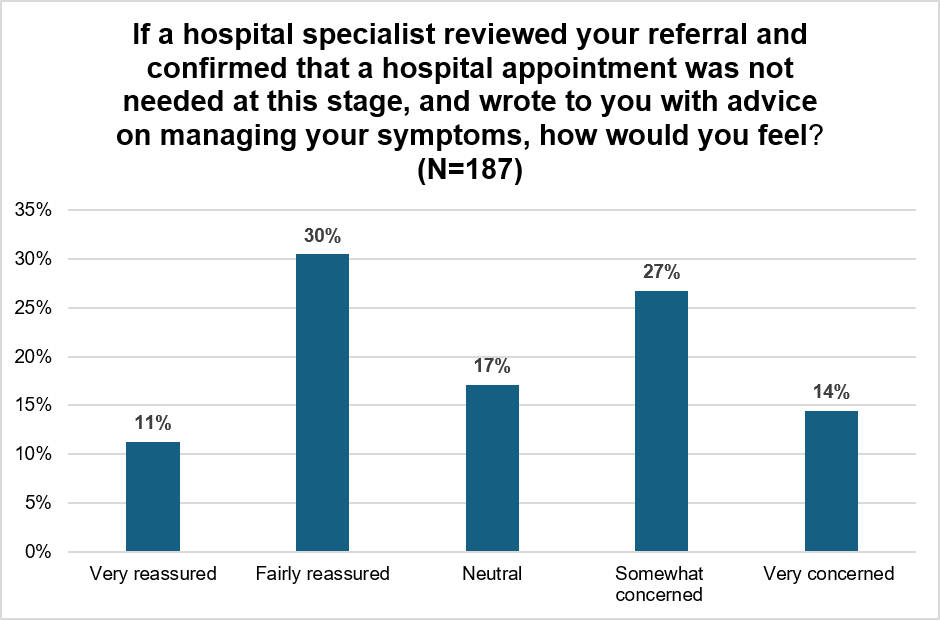
Reassurance through clinical review and confirmation. Some people value knowing that a specialist has reviewed their case, even if they are not seen immediately. This provides reassurance that the right level of clinical oversight has taken place.
Concerns about system pressures affecting prioritisation. There is a concern that prioritisation may be influenced by system capacity or cost pressures rather than purely clinical need, particularly where waiting times are already long.
Desire for holistic assessment of need and impact. Some responses highlight that urgency is not only about risk to life, but also quality of life and daily impact. There is concern that current definitions of urgency may not fully reflect lived experience and mental health will suffer as a result.
Ideas for the future – what people think should be considered
When asked what else should be considered as gastroenterology services are reviewed, people raised a wide range of issues. These included:
Clearer communication throughout the whole care pathway, not just at the beginning. People want clearer, more consistent communication at every stage of the patient journey. People describe frustration when updates are not provided, when follow-up is unclear, or when they feel left to navigate the system alone. This includes communication about referrals, test results, next steps, and changes in plans.
Better follow-up care and continuity after initial assessment or discharge. Another clear theme is concern about the lack of structured follow-up once a patient has been seen or discharged. People describe feeling that care often ends after the first round of tests, even when symptoms persist or evolve. There is a feeling that patients can be left without ongoing clinical oversight, particularly for chronic or unresolved conditions. This includes concerns that being told “nothing serious was found” can result in no further support, even when symptoms continue to have a significant impact on daily life. People also suggested having opportunities to go back into specialist care without having to start again if a symptom flares up.
Some women felt digestive symptoms were dismissed or minimised. An important theme relates to women feeling that symptoms were not taken seriously or were too quickly attributed to women’s health issues without proper investigation.
Some people felt their symptoms were normalised or downplayed because of gender, while others described concern that women’s pain or bowel symptoms were not investigated thoroughly enough. There are also examples where menopause, hormonal changes, or women’s wider health needs were not considered holistically alongside digestive symptoms.
“I’m not asking everyone to be specialists, but it would be great to feel as a woman with bowel issues that it’s not just period pains.”
Long waits, uncertainty and unresolved symptoms are negatively affecting people’s mental health and emotional wellbeing. Some people described the emotional impact of living with ongoing digestive symptoms while waiting for investigations, appointments, or follow-up care. People spoke about stress, worry, frustration, and feeling forgotten within the system, particularly where symptoms persisted over long periods without clear answers or continuity of support. Some described losing confidence in services and going private, feeling abandoned after discharge or struggling to cope with ongoing symptoms without support.
Trust, transparency and confidence in clinical decision-making. People want clearer explanations of how clinical decisions are reached, including why certain patients are prioritised over others. Some express concern about fairness and consistency, particularly when urgency decisions are not well understood. Others want reassurance that assessments are thorough and based on complete information.
Appendix One: Demographics