Introduction
On Wednesday 18 March 2026, the NHS in South West London brought together over 70 community leaders from South West London’s voluntary, community and social organisations, alongside clinical and ICB colleagues, to discuss the future of health needs and NHS services across our six boroughs. The event’s aim was to hear more about what community leaders were hearing from communities, sense check what feels most important to local people and to discuss how NHS services can respond as we move towards a neighbourhood health model.
We also looked closely at four key areas of work by clinical leaders in South West London considering long term plans for health services, responding to the national 10 Year Health Plan for the NHS.
- Prevention and early intervention
- The same standard of care wherever you live
- Improving outpatient care
- Avoiding unnecessary hospital stays.
The session built on previous conversations with communities including a listening event with voluntary and community sector organisations in January 2025, when we came together as part of the national engagement on the 10 Year Health Plan which can be read here.
After a short presentation and case studies exploring how neighbourhood care works in practice, the main focus of the session was a discussion about what community leaders are hearing from their communities and how we can work better together as the NHS shifts towards prevention, neighbourhood working and community-based care.
Our ICB Place leads then facilitated borough-based discussions on how best to strengthen neighbourhood working, asking:
- What would make the biggest difference to the health of the communities you support?
- Opportunities to work differently – Ideas about neighbourhood working, prevention, or changes to services.
Next steps
All the feedback we heard from our community leaders London at this event will help to feed into the next phase of NHS South West London’s role as a strategic commissioner. Findings will be shared with clinicians, strategic leaders and decision makers across our six boroughs. The insight from this report will help inform our approach and future plans and support the delivery of the 10 Year Health Plan across the six boroughs of South West London.
Key themes
As the NHS shifts towards prevention, neighbourhood working and community-based care, we wanted to understand the experience of VCSE organisations and the communities they represent; what would make the biggest difference to the health of communities and opportunities to work differently with VCSE organisations.
Top community concerns
When asked which themes resonated most with the communities they serve, attendees identified the following five priorities:
- Mental health and wellbeing – demand outstripping capacity and long waiting times, with particular inequalities for global majority communities and the potential for positive support in this area from the voluntary and community sector
- Inequalities and inclusion – language and cultural barriers is leading to poorer health outcomes, including increased visits to A&E and a concern around lack of access to translation services at some GP practices
- Cost of living – rising costs of living is impacting on people’s mental and physical health including maintaining basic health and wellbeing as well as people’s ability to travel to health appointments
- Referrals and waiting times – complex processes in accessing services, frequent cancellations and poor communication from some health services leaves people feeling abandoned and confused
- Support for unpaid carers – is a common concern, particularly young carers, who are described as “invisible” in some health settings.
Opportunities to work differently
Community and voluntary sector leaders discussed ways that the system could work differently and support local people and communities:
1. Whole-person, integrated care – there’s a strong call to move away from siloed, diagnosis-led care towards a more holistic model built around the person which takes into account physical, mental, social and cultural factors. The current approach is seen as too medicalised, leaving people “bounced around” between organisations. Our community leaders suggested care navigators and neighbourhood GP coordinators could help to bridge gaps and better integrate general practice with community and social care services.
“Holistic care is impossible as no one holds all the information. The way people with multiple long-term conditions are bounced around between multiple organisations who each care for individual needs.” Kingston community leader
2. Prevention and early support – community leaders called for greater consistency in preventative care, particularly while people wait for NHS services. There was broad support for the shift to prevention, and agreement that this could involve less medicalised, more holistic and community-based approaches. A key concern is that the current system only intervenes once needs reach crisis point, driven by reliance on formal diagnosis before support is provided.
“Upskill VCSE organisations in a range of interventions to provide holistic support during waits to NHS care or to prevent a need to refer someone to a separate department.” Merton community leader
3. Reducing fragmentation and improving referral pathways – the system is widely described as “too fragmented”, with poor communication causing people to fall through gaps during service transitions. There were calls to streamline referral pathways, reduce duplication, and build on what already works. Long, complex referral processes were flagged across boroughs, alongside frustration at poor communication while waiting.
“People end up all over the place with fragmented journeys.” Croydon community leader
4. Accessible information, signposting and navigation – community leaders stressed that many people don’t know where to go for help or find NHS language confusing. Trusted, accessible information with multiple access points is seen as essential. There were some borough level nuances: Kingston and Wandsworth highlighted confusion and poor signposting; Sutton raised practical barriers such as disability and mobility; Merton and Richmond pointed to trust, communication and cultural barriers; and Croydon emphasised active, VCSE-supported navigation as particularly effective.
“People don’t necessary know where to go or when for the help they need – or the cause or help they need.” Wandsworth community leader
5. Listen to lived experience and cultural change – community leaders told us that a cultural shift is needed so that clinicians genuinely listen to people, avoid assumptions, and stop labelling patients. Removing the divide between physical and mental health is highlighted, with recognition that trauma often presents as physical symptoms. Support from trusted intermediaries, particularly VCSE organisations, is seen as key to building trust with communities who currently feel “challenged rather than listened to” by NHS staff.
“People feel left high and dry by the NHS, often trust VCSE organisations more and supported by them to manage NHS routes. People feel challenged by NHS staff rather than listened to and supported by them.” Merton community leader
6. VCSE as core system partners – there is a strong call to rebalance the relationship between the NHS and VCSE sector, treating voluntary organisations as genuine partners rather than add-ons. This means involving them from the earliest stages of service design, providing direct and sustainable funding, and potentially upskilling VCSE staff to support people during long waits. Shared spaces and co-location are suggested as practical ways to strengthen collaboration and holistic delivery.
“VCSE organisations want more structured communication and partnership with the NHS – VCSE needs to be aware of the NHS priorities and have the ability to cascade throughout the sector.” Sutton community leader
Who we heard from
We were joined by over 70 community leaders from across South West London. Our Place Leads facilitated discussions in groups including community and voluntary sector leaders from each of our six boroughs alongside some of our clinical leaders. Our community and voluntary sector leaders bring with them views gathered from their work with our most vulnerable communities, they shared what they hear locally including the experiences of those impacted by health inequalities from across South West London.
We had representatives from each of these groups:
| Afghanistan and Central Asian Association Charity | Age UK Croydon |
| Age UK Merton | Alzheimer’s Society |
| Autism Voice UK | Avanti Mental Well-Being CIC |
| BAME Voice/AECHO | Balance Support CIO |
| Battersea Alliance | Bright Futures 4 All CIC |
| Cassandra Centre | Citizens Advice Merton and Lambeth |
| Citizens Advice Wandsworth | ClearCommunityWeb |
| Connect North Korea | Croydon Borough Neighbourhood Watch Association |
| Croydon Hearing Resource Centre | Croydon Sickle Cell and Thalassemia Support Group |
| Elays Network | Emmanuel Church, South Croydon |
| Family Foundations | Floating Counselling Community |
| Focus 4 1 | Friendship group affiliated to Hearing Voices Network |
| Hampton Wick Patients’ Participation Group | Healthwatch Richmond |
| Healthwatch Sutton | Healthwatch Wandsworth/WCA |
| Her, Me & ADHD | Informal Carers’ Drop-In Group Raynes Park |
| Kingston branch of Diabetes UK | Kingston Carers Network |
| Kingston Mental Health Carers’ Forum | Kingston Race and Equality Council |
| Kingston Voluntary Action | Metro Charity |
| Merton Centre for Independent Living | Merton Connected |
| Migrant Advocacy Service and Community Outreach | Milaap Multicultural Day Centre |
| Mind in Croydon | Mind in Kingston |
| Mindworks UK | Music Relief Foundation |
| Nanoom UK CIC | New Addington Pathfinders |
| Optimism Supported Housing | Places Leisure |
| Polish Family Association | Positive Network Community Project |
| Public Voice | Reaching Higher |
| Richmond AID | Richmond Borough Mind |
| Richmond CVS | Richmond EAL Friendship Group |
| Richmond Mencap | Roehampton Wellbeing for Women and Children |
| Ruils-Independent Living | South West London Healthwatch Collaborative |
| Storm | Sutton Tamil Elders Group |
| Sutton Vision | The Green Nut Community |
| Together for Mental Wellbeing | Ukrainian Social Club CIO |
| Voices of Hope | Volunteer Centre Sutton |
| Wandsworth Care Alliance | Wandsworth Carers’ Centre |
| Wandsworth Patient Forum | Wellbeing You CIC |
| Woodside Community Leader/NHS Wellbeing |
Key findings from our main discussions
To support table discussions, there was a short presentation and case studies exploring how neighbourhood care works in practice. The examples gave a flavour of how, by working better together, the NHS can shift towards prevention, neighbourhood working and community-based care.
We asked VCSE representatives to share their views on the following questions:
- What would make the biggest difference to the health of the communities you support?
- What opportunities do you see for making this work in practice?
- How could we best work with VCSE organisations and draw on your expertise?
Overall, there is support for the NHS to shift towards prevention and neighbourhood working. There is a strong perception that NHS services can feel fragmented with an overly clinical focus. People and communities would support a move towards care becoming more integrated and person-centred, supported by voluntary sector organisations helping to reach out to local communities. Key themes from our discussions are detailed below with some examples from each of our borough discussions highlighted:
What would make the biggest difference to the health of the communities you support?
Moving from siloed approaches to providing care ‘around the person’, incorporating physical, mental, social and cultural factors, would create ‘space for a range of professionals, including the voluntary and community sector, to care together for people’. Richmond organisations identified understanding cultural identity and community routines as being important to how people are cared for, whereas Croydon, Merton and Sutton focused more broadly on social determinants and trauma. It was also felt that health can be ‘too medicalised, limiting access to support’ due to focussing only on symptoms, whereas caring for the whole person would stop people being ‘bounced around between multiple organisations who each care for individual needs’.
Need for greater consistency in delivering prevention, with a stronger focus on practical early support while ‘people wait a long time for NHS care’. It’s thought this could save resources and improve outcomes, reducing long-term crises and system pressure. On the Kingston table it was noted that there can be differences in how prevention is understood – with the NHS tending to focus on stopping deterioration, while VCSE focuses on stopping issues from arising in the first place.
The current system is described as ‘too fragmented’ which impacts staff and patients when communication doesn’t work. People told us that they want to see improvements to referral pathways and a reduction in duplication to ‘stop people falling through gaps’ and avoiding unnecessarily long waits, starting with a review of what currently exists and works well elsewhere ‘rather than starting from scratch’. The Kingston discussion talked about people’s experience of long waits for care and how services were not joined up enough to support the individual. Croydon, Richmond and Sutton discussions focussed more on the importance of preventing inappropriate demand and supporting people to be seen in the right place, at the right time.
Easily accessible trusted information and signposting is viewed as being essential, with many people not knowing where to go for help or struggling to understand the language used ‘what is strategic commissioning?? What is neighbourhood??’. It’s suggested that co-locating health workers within voluntary and community sector organisations could also help people to access support by raising awareness of services.
Clinicians to hear and be led by lived experience , requiring ‘a change in culture to genuinely listen to people, stop making assumptions and labelling them’. A call to ‘remove the divide between physical and mental health’ was also made, noting trauma manifests as physical issues ‘driven by people needing someone to talk to immediately’.
What opportunities do you see for making this work in practice?
Move to needs-led care around the person rather than diagnosis-led: With long waits ‘causing frustration’, it’s thought that cross-sector collaboration through care navigators or Neighbourhood general practice co-ordinators would fill the gaps for people who need it while it was felt that ‘GPs are disconnected and communication isn’t good enough’. This would ‘integrate general practice with community services including social care’ connect people to a community specialist in the appropriate area, once seen by the GP, to be provided ‘support, test results etc when GPs are unlikely to have capacity’.
Help to join up the NHS to make it easier to navigate by improving the networks between NHS, social care and VCSE organisations. It was suggested that this would ‘help professionals and patients navigate processes’ and support people’s care by joining up services. Wandsworth’s table discussion looked at the limited time GPs have to be able to support patients holistically during short appointments, and other boroughs talked about improving the links between NHS services including with the support of the voluntary and community sector.
Support from trusted intermediaries including the voluntary and community sector
in navigating and understanding about the NHS and health care is thought to increase people’s understanding and helps to strengthen trust, compared to sometimes when people can ‘feel challenged by NHS staff rather than listened to and supported by them’.
Shared and consistent signposting were flagged as important, with messaging spread by engaged individuals as people ‘feel left high and dry by the NHS and don’t know how to get hold of support’. Navigation, information and access challenges were raised by all boroughs as impacting access to health services, but each with a different emphasis:
- Kingston and Wandsworth organisations stressed confusion, poor signposting and lack of awareness
- Sutton organisations emphasised practical access barriers such as disability, mobility and lack of service responsiveness
- Merton and Richmond organisations highlighted a lack of trust, communication and cultural barriers
- Croydon organisations focused on the voluntary and community sectors role in supporting people to navigate local services and healthcare information.
How could we best work with VCSE organisations and draw on your expertise?
Rebalance the structure to treat the VCSE sector as core system partners with early involvement and inclusion. The NHS is urged to ‘listen to community organisations to see the value in co-production’, for example when designing a new service to ‘involve potential partners from the start of conversations/planning – you can’t design a service if you don’t really understand it’.
Enable VCSE organisations to play a key role in improving access and experience: The VCSE sector is seen as possessing ‘significant skills’, but it’s identified that ‘we (NHS) have to be willing to pay for them’. For instance, ‘give direct funding where it’s felt more possible to make impactful actions’ such as charities which are ‘more attractive to vulnerable groups such as children to go to for support’ as not part of an institutional set-up. It’s also suggested that upskilling VCSE organisations in a range of interventions would support people during long waits for NHS care and prevent people needing to be referred to separate departments.
Create an integrated and culturally sensitive culture of ‘working together to help all to understand the value in each other’. It’s thought shared spaces or hot desking in community locations would ‘strengthen collaboration, visibility and holistic delivery’.
What is important to communities?
The final discussion focused in on what our communities are thinking and feeling, not just about their health, but about what is going on in their broader lives too.
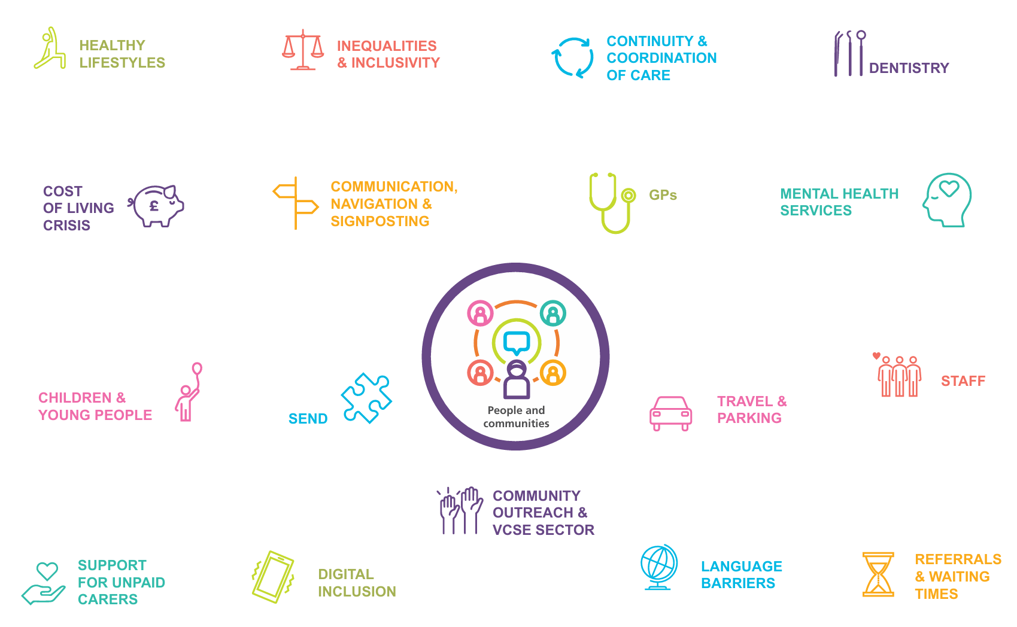
Attendees were presented with an infographic (see above) that summarises some of the key themes that have been coming out of the engagement work the ICB has been doing over the past year. These themes were a result of 1,000s of conversations with local people – focusing on inequalities in our communities and capturing barriers to accessing care. It brought together insights from across partners – including Healthwatch and the voluntary and community sector to learn from each other – and build a shared understanding of what’s important and avoid asking people the same questions.
We asked each table to rate the themes according to how far they resonated with the communities they support.
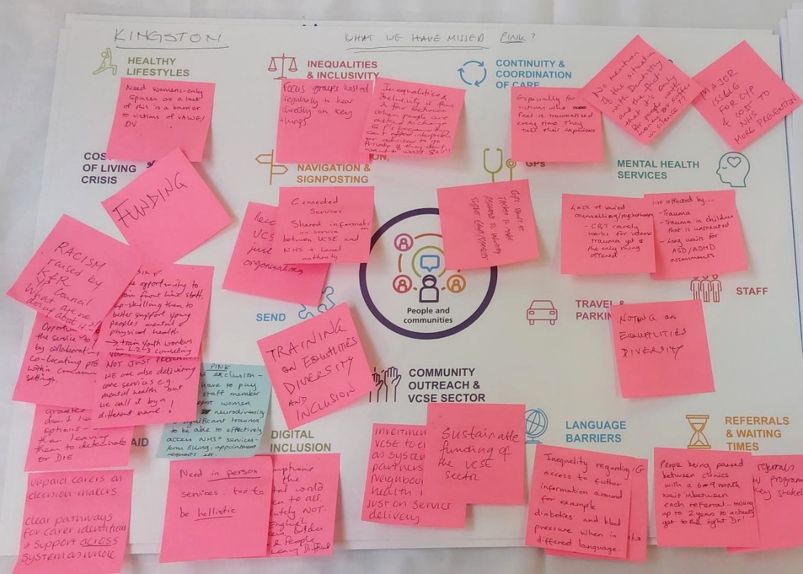
They were also asked to identify any missing themes.
Themes that resonated most with attendees
Across all boroughs, we heard that the following 5 themes resonated the most in their communities:
1. Mental Health
Mental Health resonated highest with the needs of communities across all boroughs. Discussion identified concern that demand for mental health care is outstripping capacity and that waiting times are too long. Community leaders also see clear inequalities for those from global majority communities in both the perception of mental health issues as well as in accessing services. Potential opportunities were also highlighted to work more closely with VCSE organisations to help support local people with their mental health and wellbeing needs.
- “VCSE has many interventions which can reduce or prevent waiting lists e.g. EMDR, trauma informed services, crisis support, peer support.” Richmond discussion
- “Waiting times for secondary care are too long – people are waiting so long that circumstances change and people go into crisis.” Croydon discussion
- “MH and LD services need to be separated. Adults with LD struggle to get MH support.” Richmond discussion
- “Increase investment in befriending to reduce isolation and give mental health support.” Sutton discussion
2. Inequalities and inclusion
People also identified issues of inequalities and inclusion across all SWL boroughs. Negative consequences are felt to arise from a lack of support in accessing healthcare for those who don’t speak or read English, including increased A&E attendances, further driven by inaccessible translators at GP appointments. Increased negative outcomes for global majority communities was also highlighted.
- “Health inequalities – obvious across SWL.” Merton discussion
- “People are asked to change GPs because they can’t afford interpreters or advised to go private if they don’t want to wait: sad!” Kingston discussion
- “Language and culture are barriers to access. More understanding of this.” Richmond discussion
3. Cost of living crisis
The rising cost of living was said to be reducing people’s ability to look after their health and wellbeing, from not being able to access gyms and nutritious foods to preventing travel to appointments.
- “Cost of living significantly impacts access to healthcare and wellbeing” Croydon discussion
- “Examples include no heating, turning off pressure relieving equipment due to cost, and cost of travel to appointments” Wandsworth discussion
- “Not all NHS services are free – Pharmacy, dentistry, ophthalmology and cost of living affects these” Croydon discussion
- “More joined up work on cost-of-living crisis in the borough. More investment.” Kingston discussion
4. Referrals and waiting times
Long waits and frequent rescheduling/cancelling of appointments were raised as another key concern. Referral processes were described as ‘complex’, further creating barriers for some.
- “Need support to be communicated with information while waiting. The health system only updates you once appointments are confirmed; not much in between.” Wandsworth discussion
- “Recent cancellations leading to delays; feeling abandoned, frustrated, in pain.” Wandsworth discussion
- “Complex referral processes and long waiting times create barriers.” Merton discussion
- “People being passed between clinics with 6-9month wait in between each referral – taking up to 2years to actually get to the right doctor.” Kingston discussion
5. Support for unpaid carers
People also identified support for carers as a key need across South West London. Specific support tailored to young carers, increased resources and improved access was highlighted.
- “Government financial and social support for carers is very limited.” Richmond discussion
- “Support for unpaid carers.” Sutton discussion
- “Young carers are invisible in health settings, ignored, patronised.” Wandsworth discussion
Additional themes
These conversations also revealed additional themes said to be of importance to communities in SWL:
Women-specific services
People identified a need for women-specific services to be provided as standard, with ‘safe spaces’ so that all women, including those who are vulnerable, feel supported to access health and fitness resources. There was also a call for more community support for common women’s health conditions to increase access.
- “More community support for Women’s Health conditions endometriosis, fibroids etc.” Sutton discussion
- “Women-only spaces for victims of domestic violence.” Kingston discussion
- “Need for women only services to be offered as routine.” Richmond discussion
Safe and affordable housing
The lack of safe and affordable housing in south west London was raised as a concern, recognised as an important determinant of health in playing a preventative role in supporting good physical and mental health. A lack of support for people who are or face street homelessness was also discussed.
- “Housing crisis – no collaborative working with VCSE orgs, local authorities and clinical teams – rehousing and homelessness.” Croydon discussion
- “Housing safe affordable would reduce health needs.” Merton discussion
- “Support for people who are street homeless inc with vulnerabilities and families.” Croydon discussion
Better understanding of prevention
People called for greater clarity on the meaning and aim of ‘prevention’. There is confusion as to whether the term refers to a focus on early intervention to prevent deterioration, or whether it instead refers to preventing issues from arising. However, people agree that prevention should involve opportunities for less medicalised care, looking instead at holistic ways of caring for people.
- “Better understanding of what prevention means.” Richmond discussion
- “Need for early support, including non-medical and community-based interventions.” Croydon discussion
- “Prevention – the need for information to be based on experience of those with a condition.” Kingston discussion
Barriers to prevention
Concerns were raised that the current NHS system doesn’t allow for early interventions, meaning people’s needs can increase while waiting to be given support.
- “Lack of early interventions.” Wandsworth discussion
- “Current systems rely heavily on formal diagnosis before support is provided.” Merton discussion
- “Conditions have to reach crisis points before support given.” Wandsworth discussion
Further detail about discussions by borough is available upon request.